

Heterogeneity in Autism and How Science is Addressing It
A summary of autism research in 2017 and what it means for families
By Alycia Halladay, PhD, Chief Science Officer of the Autism Science Foundation and the Scientific Advisory Board of the Autism Science Foundation
To listen to our year-end science summary podcast, click here.
![]() This was not the first year that understanding the different subtypes of autism became a hot topic of discussion in the autism community, but in 2017, it certainly had much higher visibility on community blogs, in public speeches, editorials, science surveys, and public forums. There was especially fierce debate on the specific needs of people on the spectrum across the lifespan, with some divergence on the priorities of research.
This was not the first year that understanding the different subtypes of autism became a hot topic of discussion in the autism community, but in 2017, it certainly had much higher visibility on community blogs, in public speeches, editorials, science surveys, and public forums. There was especially fierce debate on the specific needs of people on the spectrum across the lifespan, with some divergence on the priorities of research.
The US Government Makes a Plan
Generating some of this discussion was the new strategic plan of the Interagency Autism Coordinating Committee (IACC). The committee, which is authorized by the Autism Cares Act, reconvened in 2015, but began work on a strategic plan for science this year. The IACC is made up of both public and private members representing funding agencies, advocacy organizations, people with autism, service providers, parents, and researchers, all members of the autism community. The group provides advice to the Secretary of Health and Human Services, collecting information from a wide variety of audiences to identify top priorities and needs in autism research. Importantly, the IACC does not make funding decisions, but the federal government uses its recommendations as a guide for calls for funding and other funding opportunities1.
Credit: National Institutes of Health
The IACC also writes a strategic plan for autism research each year, which guides but does not mandate funding opportunities. An updated IACC strategic plan published this year, reformulated seven crucial questions of importance for the autism community. It included an entire chapter devoted to meeting the needs of individuals as they move into adulthood, clearly an understudied and underfunded topic. The revision and expansion of this chapter sparked debate on what precisely those needs are.
Different Perspectives and Priorities
Surveys and interviews in the United Kingdom have revealed differences in the research priorities of different stakeholder groups2,3, and this year Autism Speaks conducted an online survey of its own4 which showed somewhat similar findings. As a whole, self-advocates and autistic adults place less of a priority on understanding early symptoms, biological mechanisms, causes, and treatments than parents. In addition to more formal findings in scientific literature, voices expressed via the blogosphere revealed highly disparate opinions of self-advocates5 and parents6. These differences may be partially explained by the differing abilities and disabilities of adults who are able to express their needs and voice their opinions and those who rely on parents or caregivers to do so.
But what does the science say? Qualitative research has revealed that autistic adults feel that research directed at changing them is counterproductive, and that adaptation needs to occur in the world around them3. Understandably, research priorities are also driven by individual personal experiences with individuals with autism and autistic adults7,8. While the goal of the DSM 5 was to provide a more accurate and specific diagnosis, an unintended consequence has been to lump the differently able autism groups into one definition, sometimes creating confusion and resentment when limited research money is involved.
Unfortunately, developing specific ways to distinguish the different subtypes of autism across the spectrum has proven elusive and remains one of the big challenges of autism researchers. Current large-scale research projects are focused on using biological approaches to distinguish the different subtypes. The subtypes will be used to understanding the different causes, to understand different strengths and abilities along with needs and disabilities, and to develop more focused, personalized treatments. These subtypes may be based on how individuals function in society.
This year, given new initiatives in sharing, pooling and standardizing larger data sets, researchers were able to re-examine the differences in autism phenotype, called the “autismS,” scientifically. The goal of identifying different subgroups of individuals with autism and autistic adults is to better characterize their needs and abilities toward tailoring services and supports, because the needs of each person can be so drastically different across the spectrum.
The Big Way the Ends of the Spectrum Are Different From Each Other
One factor that discerns both those who are able to self-advocate and those who need ongoing lifetime care is cognitive ability, measured by intellectual quotient or IQ. To truly understand the variability of people across the autism spectrum, big data is going to lead scientists to more answers.
This year, scientific research articles examined the different outcomes of individuals with autism with a wide range of cognitive abilities and found that IQ was an important predictor of outcomes in children with autism9-12. These included children involved in treatment studies as well as research cohorts. This is not necessarily a new finding, but it does replicate findings in larger cohorts that had previously only been replicated in smaller studies.

In these studies, autism severity scores, adaptive behaviors, and communication improved in individuals with higher IQs12; those with lower IQs typically had the highest severity symptoms10. Additionally, while stability of an autism diagnosis is high, children with autism who did ultimately move off the spectrum after diagnosis were more likely to have an average developmental quotient, reflecting higher cognitive ability13. Of course, early intellectual quotient does not fully explain outcome11, as language ability is also crucial12. It is also important to note that although cognition is often intact in individuals with optimal outcome, IQ alone does not always result in independent functioning. In other words, IQ is not the be-all-end-all of outcome in autism. As revealed in the Autism Speaks Autism Treatment Network, many individuals with ASD who do not have cognitive impairment exhibit significant deficits in adaptive functioning, and this gap has again been found to be larger in older versus younger individuals14. These differences can be associated with psychiatric comorbidities into adulthood15. These findings highlight the need for evaluating, monitoring, and treating adaptive behavior over time to determine whether an individual is independently applying her repertoire of cognitive skills to daily routines and activities when life demands them. The most comprehensive measure for assessing adaptive behavior is the Vineland Adaptive Behavior Scales, now in its Third Edition16, which helps clinicians better assess the role of adaptive behavior in both symptoms and a multitude of outcomes associated with autism.
Other larger scale studies to subtype children with autism have revealed that more subtle language use and language impairments do a good job of distinguishing different groups of people with autism, and that these groups also differ in non-verbal IQ17. In the Study to Explore Early Development, a project that included almost a thousand preschool children with autism, clinician scientists explored how symptoms cluster together to form groups, which may be then used to describe subtypes. Factors such as language impairments and cognitive rigidity predicted who was in what subtype18. This is the largest study so far to look at different aspects of functioning and abilities in a group of children with the intention of trying to group them into different types.
Beyond “Yes or No” as a Diagnosis
But why look at an autism diagnosis as an either/or thing when there is so much that distinguishes people across the spectrum? Rather than considering autism a “yes or no” diagnosis, there is now more evidence from larger groups that there are different dimensions of autism symptoms in children, including language and cognitive ability18. It is less about presence or absence of intellectual disability and language, but language and cognitive abilities along a continuum of impairment. Cognitive ability may also play a large role in autism diagnosis. A recent prospective study of the DSM-5 reinforced the high sensitivity and specificity of the newer DSM-5 criteria, while also revealing that those with higher IQ who were labeled under DSM-IV may not have met the threshold for an autism diagnosis under the DSM-519. Taken together, these studies further add to the research published this year that demonstrate different features of autism may constitute different types of autism, or new forms of autism altogether.
Efficacy of different intervention strategies also seems to be dependent on IQ of the child, as a scientific analysis of the anecdotal reports of fever improving symptoms was investigated. Parents with a child with lower non-verbal IQ and lower language levels reported more fever-related improvements in communication and repetitive behaviors20. This could be explained by multiple factors, including the presence of a definable subtype that is more responsive to different interventions.
The Biology Behind Autism Subtypes
Credit: Susanna M. Hamilton, courtesy of Broad Institute
Large-scale genetics studies of thousands of individuals with autism showed that different autism subtypes also have distinct genetic profiles. For example, those with what is known as a de novo mutation (not present in mother or father), show lower IQ scores and higher rates of epilepsy than those with what are known as common variants21. Therefore, different types of genetic mutations can have different influences on autism symptoms and can work together to shape different features of autism. Common variants, which can be inherited, are seen in everyone, but add together to increase risk of certain diseases like Alzheimer’s and Crohn’s. They do not seem to influence intellectual function in autism, while de novo variants do21. Whole genome sequencing studies also showed the diversity of different types of genetic variants in people with autism.22 While the association of de novo variants with lower IQ in individuals with autism is not a novel finding, the replication across multiple large-scale studies is an important contribution.
Adding to the complexity of the role of these de novo mutations, researchers discovered that when those with and without de novo mutations were matched based on IQ, those with de novo mutations actually have less pronounced autism symptoms23. Therefore, these finding suggest that these mutations may not confer any more risk for autism than other types of mutations. In other words, they may be more indicative of IQ than they are of autism. In addition, those individuals with de novo mutations had a different pattern of brain activity when shown non-social vs. social video scenes, independent of cognitive ability24. In fact, in some analyses, for people with autism and de novo gene mutations, intellectual disability is treated as a co-morbid symptom rather than a subtyping measure25. This again shows the differential influence of de novo gene mutations and other types of mutations on autism symptoms, and the importance of taking IQ into account when understanding autism and that presence of intellectual disability, presence of de novo variants, or both, may be a distinct autism subtype.
Big data, or large sample sizes, also helped scientists understand how an autism diagnosis influences immune functioning on a genetic level26 and has helped resolve discrepancies in findings in brain structure across studies. In fact, the largest study to date of people with autism at different ages illustrated that the cortex is most enlarged in adolescence, and replicated findings that other areas like the nucleus accumbens (moderating reward) and the amygdala (controlling emotion and anxiety) were smaller in those with autism27. The ultimate in “big data,” whole-genome sequencing, revealed new genes of interest and greater appreciation for the role of these genes. For example, one group found that previously understood areas of the genome, previously unstudied, could be important for ~6% of autism diagnoses22.
Presence of mutations in newly identified autism risk genes were also associated with lower adaptive ability, furthering the notion of a more severe genetic phenotype, as suggested earlier28.

With new datasets, it is also possible to determine the origin of when the de novo mutation occurred. As these de novo mutations occur in a small percentage of people with autism, large numbers are needed to better understand their influence and role in diagnosis. These different types of mutations can occur prior to the formation of the embryo, or in the post-zygotic period after the formation of the embryo. The timing of these mutations seems to have influence over behavioral features24 and has also been linked to the development of specific brain regions, specifically the amygdala29. There is also preliminary evidence to suggest that individuals with these post-zygotic mutations are less likely to be intellectually impaired29, again tying genetics with intellectual function and autism diagnosis. These post-zygotic mutations are present in a significant percentage of individuals with autism30, making them a potential target for new personalized medicine initiatives.
Genetics Provides More Answers
The genetic influence on specific behaviors, particularly autism-related behaviors, was better understood this year. By looking at twins, researchers were better able to establish the genetic influence of specific autism behaviors, specifically different eye gaze, which describes how people with autism pay more attention to objects and less to social situations31. This behavior controls how people with autism take in information about the world around them. Under strong genetic influence, eye gaze is altered in people with autism, and this differential input of different exposures then influences brain development. As Warren Jones, an author or the study stated, the effects of genetic influence on behavior “ripple forward” to alter brain development.
Genetics have also helped explain the comorbidity of autism with psychiatric issues and disorders. While behavioral overlap is seen between autism and disorders like schizophrenia, ADHD and anxiety, there have been few studies that identify a genetic overlap. This year, a novel locus on chromosome 10 was identified through large scale collaboration of multiple genetic cohorts32. With regards to schizophrenia, the exact symptoms and the mechanisms of schizophrenia and autism are not identical. But what causes the difference? To investigate, researchers used a sample of over 5000 individuals to determine the overlap between social communication symptoms in both autism and schizophrenia. It seems as the genetic influences of social communication features in autism and schizophrenia may be based on development, with one genetic factor being more prominent in early development (autism) and the other in adolescence (schizophrenia)33.

Credit: FamilieSCN2a Foundation
Beyond psychiatric comorbidities associated with autism, one of the concerns of both families and autistic adults is presence of medical comorbidities, such as epilepsy. A large percentage of people with autism have some form of epilepsy, but not everyone with epilepsy has autism. So is there something different about epilepsy in people with autism? In order to address this, scientists focused on the SCN2A gene, which codes for a sodium channel that can mediate the activity of a neuron34. Research using genetic, molecular and electrophysiological data showed that very tiny variations in the way this channel works may be at the center of these differences. Some mutations in the way the sodium channel functions are associated with epilepsy in the absence of autism, another type of mutation on this same gene which controls the same sodium channel is associated with epilepsy as a comorbid disorder to autism34. This opens up possibilities to both better understand autism and epilepsy, and how to treat the specific features of epilepsy in people with autism.
Other major breakthroughs were made using animal models to understand the molecular underpinnings of autism, providing new hope for novel drug treatments. For example, individuals with mutations of a specific region of chromosome 16 have a high risk of autism. A better understanding of genes on this chromosome could lead to more targeted treatments. One of these genes, KCTD13, was found to be crucial to the changes in synaptic plasticity associated with mutations of chromosome 16, and most importantly, these changes were reversed with a compound that inhibits a chemical called RhoA35. In another study, behavioral features following a particular mutation in the tuberous sclerosis gene in mice was shown to be similar to those with autism. These features were controlled by a particular cerebellar circuit, one that could be turned on and off in the animal model36 and rescued some of the behavioral features. Taken together, these exciting findings illustrate the capacity for new medical or pharmacological interventions to treat not all of autism, but particular symptoms determined in part, by the presence of different genetic mutations.
It’s Not All Just Genetics

Genetics is not the entire story in autism, and scientists continue to identify environmental factors that work together with genetics to confer risk, and through that, to identify ways to preempt symptoms, especially in those most disabled. In 2012, the first study appeared suggesting that maternal consumption of folic acid prior to pregnancy and during pregnancy reduced the probability of having a child diagnosed with autism. This year, two new large epidemiological studies in the US and Europe replicated and expanded these findings, showing a lower probability of having a child with autism after folic acid use37 during pregnancy, and more specifically, a child with autism and intellectual disability38. A meta-analysis of multiple studies showed this effect was not limited to one particular race or ethnicity39 and is present regardless of whether there was a strong genetic or environmental component to the diagnosis37,40. The recommendation to take folic acid prior to or during pregnancy is not unusual—it’s something that the March of Dimes has been telling women to do for decades to reduce birth defects. Also, gene/environment interactions, rather than the influence of one or the other, have again proven critical. Presence of a genetic mutation called a copy number variation, plus exposure to high levels of air pollution, showed an effect on diagnosis more than either by itself 41.
This year, the presence of gene/environment interactions was, for the first time, explored in terms of autism symptoms rather than probability of autism diagnosis. Rather than examine each genetic mutation individually, researchers examined environmental exposure with type of genetic mutation—either copy number variation or mutation—in likely autism genes. Two studies revealed that the combination, rather than each in isolation, increased autism severity scores in children with prenatal exposures and genetic factors42,43. This approach will open the doors to new ways to understand genetic and environmental contributions together, rather than in isolation, on different autism outcomes.
Some environmental factors have been shown to increase probability of a diagnosis in the absence of genetic susceptibilities. One such risk factor, maternal immune activation in response to an infection, has been shown to raise the probability of having a child with autism up to two-fold. This year, toxoplasmosis and herpes were added to the list of possible immune events that can increase risk44,45. More importantly, the mechanism by which maternal immune activation alters probability of diagnosis was better ascertained. While previous studies have hypothesized through animal models or epidemiological designs that circulating chemicals called cytokines, produced as a response to maternal immune activation, were the cause, newer findings in the cerebral spinal fluid in individuals with autism and autistic adults has not found this to be the case46. Rather, transcription of genes that control how the brain is connected and shaped during development can be altered with early immune activation47 and is thought to be more crucially involved. And it isn’t all forms of maternal immune activation, as the presence of fever specifically as part of the immune reaction is also an important component of the effect48.
Another environmental factor, spacing of pregnancies, was also replicated as a risk factor in a large study. Too little time or a large amount of time between pregnancies increased the risk of the second child having an autism diagnosis49. Better understanding of the mechanism by which this occurs could lead to factors that could preempt symptoms49.
Of importance to the community, some environmental factors have been dispelled as influencing a diagnosis. For example, new and advanced statistical techniques have unraveled the role of maternal depression from maternal antidepressant use, and found that the use of antidepressants itself was not sufficient to elevate the probability of having a child diagnosed with autism50. Also, rather than infertility treatments, infertility itself seems to be underlying the link between in vitro fertilization and autism51. Understanding of these relationships allows parents to have more informed conversations with their doctors about family planning.
Paternal and Grandparental Factors
Environmental exposures aren’t just a “mom thing,” either. Paternal exposures are also known to play a role. Both maternal and paternal prenatal exposures to asthma- causing agents have also been shown to be linked to autism52. Advanced paternal age, linked to autism in multiple studies previously, was also more carefully examined. The same researchers who studied the association to autism also quantified factors in older fathers that led to higher educational achievement in kids, and named them in aggregate as the “geek index53.” Those fathers with a higher “geek index” were more likely to have male children who went further in school and earned more money53. This outcome is clearly different from those with lower functioning autism, who may not be able to be independent. This shows that there are different pathways originating from the same place, which are associated with different outcomes. Paternal influence on outcome might possibly be explained through epigenetic mechanisms—the way environmental factors turn on and off genes during development. Exposures prior to pregnancy might affect both the sperm and egg of future generations, seen when there is a paternal effect. These changes in gene expression have been linked to a number of outcomes, including autism. They are not just observed in parental exposures, but in grand-parental exposures as well. These types of observations are incredibly hard to achieve, since outcomes need to be tracked across generations, through many decades. However, use of registry data or longitudinal studies where databases are linked on related individuals now makes this possible.
This year saw the first study of grand-parental exposure on later autism features. Grand-maternal smoking was linked to impaired scores on social communication measures and restrictive and repetitive behavior scales, which are independently predictive of an autism diagnosis54. Not only is it the first study to look beyond mother/father exposures, because this grandmaternal exposure affects the egg or sperm of subsequent generations, these findings advance the role of epigenetic mechanisms involved in autism. These include methylation, where methyl groups that are attached to areas of the DNA turn on and off gene expression, and histone acetylation, where DNA winds on histones, which may affect gene expression. Late last year, a project that investigated the cumulative effects of genetic mutations with environmental exposures was conducted in cell lines. This study showed new methylation marks on even more autism risk genes, which may cause genetic instability in areas of the genome outside the original mutation55. This opens up new ways to understand the role of genetic and environmental contributions to autism. However, because epigenetic marks are dependent on the tissue of interest, studying the brains of people with autism is essential to better understanding underlying causes of ASD.
It Takes Brains to Solve Autism
Credit: Ruth Weir, UC Davis MIND Institute
The Autism BrainNet provides brain tissue to researchers worldwide to not just discover the causes of autism, but also identify newer treatment targets, and pinpoint the underlying neurobiology of autism to better understand individuals with autism. The largest study to date on methylation in autism found greater levels of methylation in autism brains compared to those without autism, across the genome but also in particular patterns of DNA regions56. Looking more specifically at particular neurons in the cortex, areas that are more or less methylated in autism compared to those without autism were focused on the immune system and neurodevelopment57. Taken together, differential patterns of methylation in brain tissue may explain gene / environment interaction in autism.
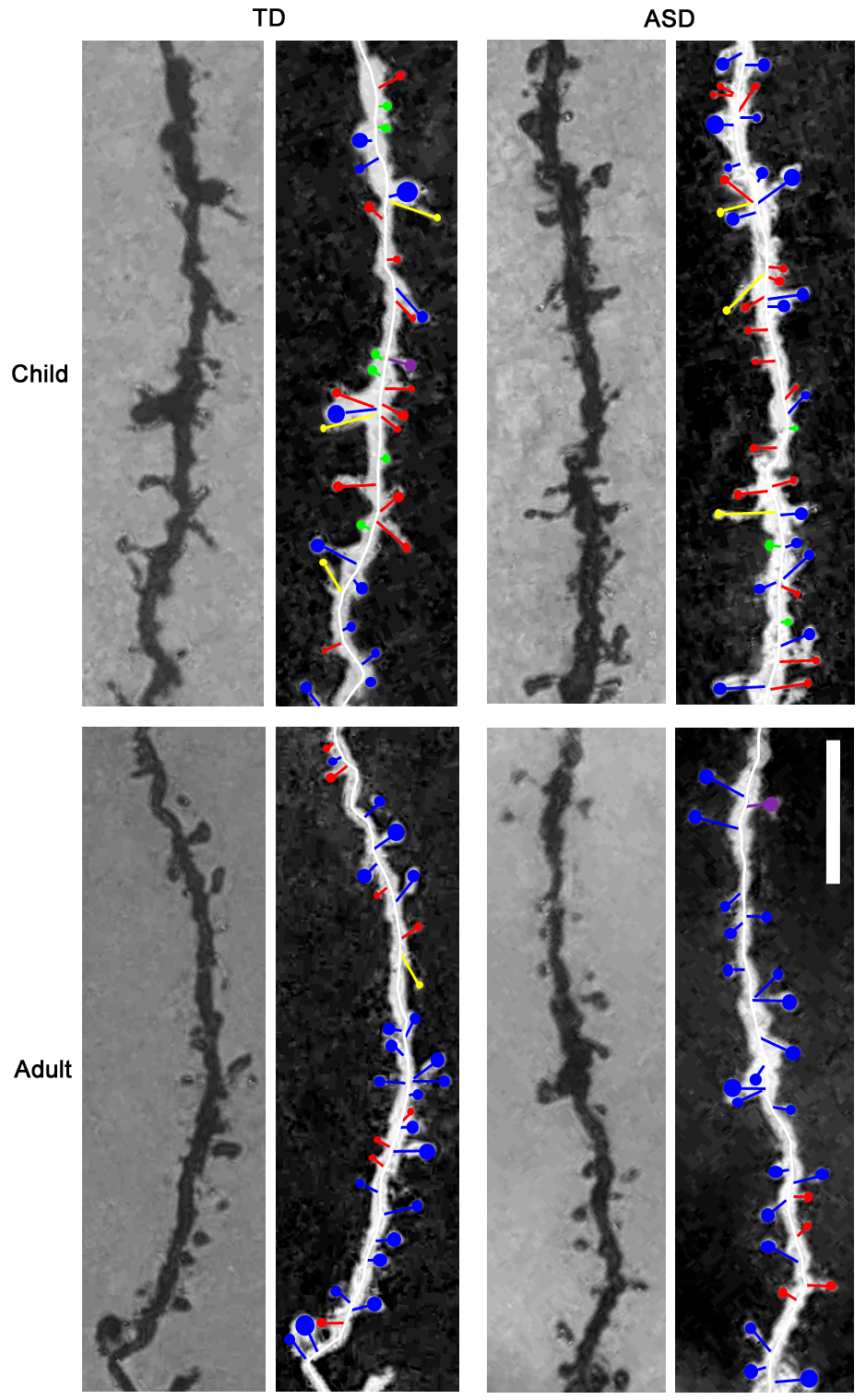
But the autism discoveries, which are possible thanks to brain tissue, are not limited to causation. The region called the amygdala has been linked to autism through genetic, behavioral and structural neuroimaging studies. Looking at the cells in the amygdala, researchers find that the neuron length is longer and there are more sites of contact with other neurons on them in the autism brain58. However, these changes are age-dependent, as there are greater spine densities compared to controls in children and adolescents and less density compared to controls in adulthood, which may partially explain changes in symptoms of autism as people age58. Another clinically relevant finding is the loss of what are known as inhibitory neurons in the cortex of brains with autism. A decrease in signals that slow down neuronal activity in the brain may contribute to the dysregulation of too much or too little activity in multiple areas brain examined by different research groups59,60. In addition to a reduction in inhibitory neurons which help with the checks and balances of brain activity, there is evidence that cells that become neurons of the corpus callosum, the tract of fibers that connects the right and left hemisphere, do not develop properly 61. This is consistent with other studies using imaging techniques, which demonstrate that cells in the brain do not go to the right places or do not reach their final destinations accurately. These results also help explain some of the behavioral and biological signs of ASD.
The Big News This Year: Biology Before Behavior
Credit: Jason Wolff, University of Minnesota
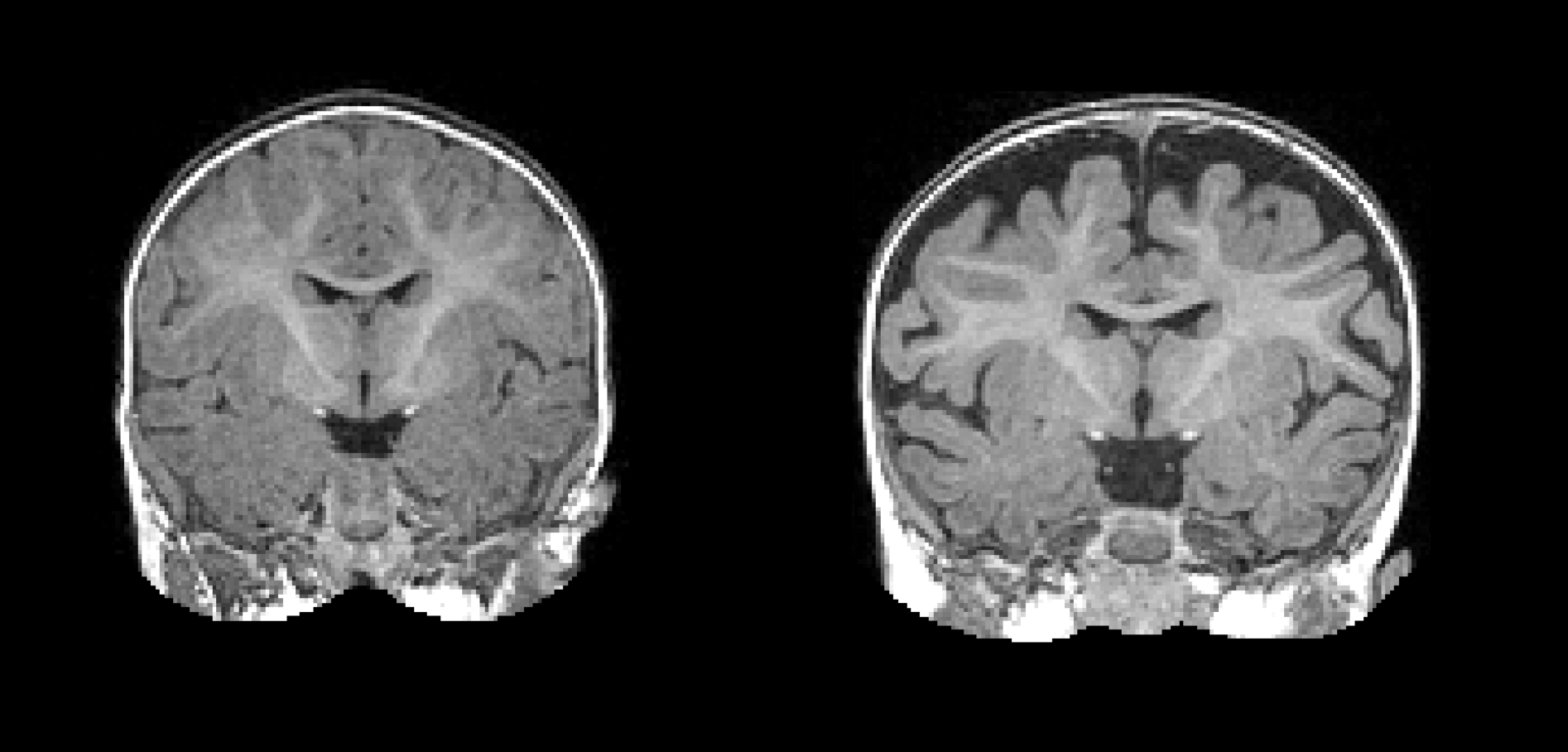
Some of the most highly-publicized and possibly the most impactful findings from this year were multiple studies that looked at early biological signs, or biomarkers, of autism before autism symptoms emerge. One longitudinal research study, called the Infant Brain Imaging Study, tracked brain size and shape of infant siblings of those with an autism diagnosis, who have a 15x risk of being diagnosed themselves. In this way, biological features from as young as 6 months of age were tracked in infants to 2 years when autism diagnosis could be made. This allowed scientists the unprecedented ability to detect biological features prior to when even very early warning signs emerge, with the potential for even earlier detection and, hopefully, earlier intervention.
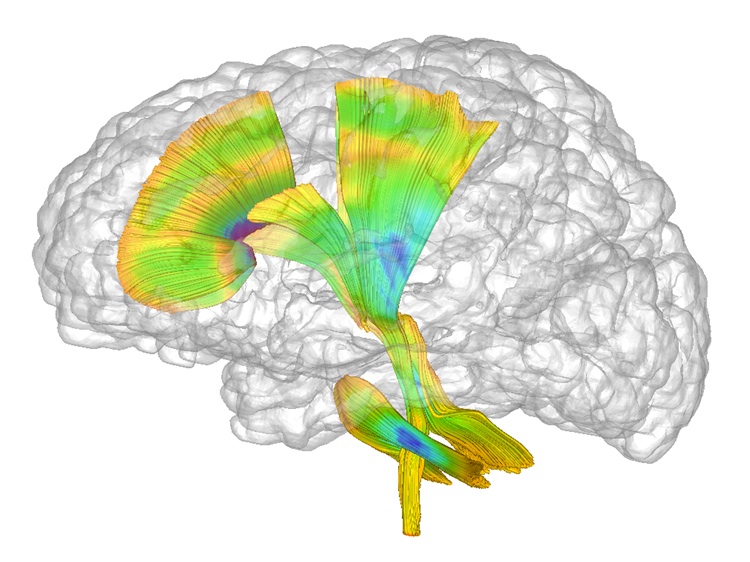
Earlier findings from the Infant Brain Imaging Study revealed that white fiber tracts grew at a slower rate in infants with autism compared to those who did not. While interesting, those findings were also preliminary. This year, a more detailed analysis of growth in infants with autism showed that increased surface area of the cortex from 6-12 months was tied to brain overgrowth at 12-18 months, which was then associated with social deficits62. The researchers then took this larger data set—MRIs of brain volume, surface area, cortical thickness at 6 and 12 months of age, and gender of the infants—and used a computer program to identify a way to classify babies most likely to meet criteria for autism at 24 months of age62. Now scientists are even closer to finding a biological method of detecting autism even before behavioral features emerge in babies with an older sibling with autism.
Credit: Mark Shen, University of North Carolina at Chapel Hill
This finding was followed by the discovery in the same dataset of the use of 6 months functional connectivity as an accurate predictor of autism diagnosis63 and identification of the circuit that controls a key feature of autism—joint attention64. Functional connectivity analyses at 6 months also revealed a different circuit for the emergence of repetitive behaviors and sensory sensitivities65. Later in the year, another analysis of the data revealed an 18% increase in cerebrospinal fluid outside the brain could be detected in those with autism as early as six months of age66.
While the Infant Brain Imaging Study was used to generate algorithms for earlier diagnosis, other investigations also revealed different interesting biological markers that need further study. For example, electroencephalographic (EEG, a measure of brain activity) markers in the frontal lobe of the brain were altered in three month-old infant siblings of those with autism, compared to those without an older sibling67. Another research group showed that, at seven months, EEG during a gaze shifting task improved the accuracy of a commonly used instrument to detect early signs and symptoms of autism in infants, the Autism Observational Scale in Infants68. This suggests that biological measures can enhance behavioral observation to predict ASD. At 18 months, compared to toddler siblings of those without an autism diagnosis, younger siblings of individuals with autism exhibited less synchronized activity between both sides of the brain. These infants showed higher levels of sensory seeking, which was linked to autism symptomatology69. This may open the door for earlier interventions focused on particular symptoms, reducing disability.
New Early Markers of Autism
Current larger scale studies are now examining the use of EEG as a biomarker for autism and how it is linked to symptoms. The convergence of data around neurological signs of autism, before even the time when symptoms are able to be detected by a trained clinician, shows the importance and power of infant siblings research design to identify the earliest biological signs. Earlier detection leads to expedition into early intervention. But it wasn’t just about biology. Another, even earlier, behavioral marker was revealed this year. This was to name which, when not present by nine months, predicts an earlier diagnosis of ASD and lower receptive language scores70. Pediatricians should be urged to consider this as an early warning sign of ASD.
The Autism Community Takes Part
The same biological markers used to aid in early detection of autism are also helping to understand how early interventions are affecting brain function. Following very early exposure to a parent-delivered intervention for those who have a 15x higher probability of an autism diagnosis (infant sibs), some of the brain activity markers changed within months after the intervention. This shows that parent-delivered interventions help to change both behaviors and brain function. And while parent-delivered interventions don’t necessarily lead to a change in autism diagnosis as a “yes or no” concept, longer term follow up of early infant interventions have, again, resulted in positive findings with regards to attentiveness and initiation of communication71, which may lead to even greater gains with longer follow-up, or higher level of functioning in those with a diagnosis. Of great importance to advocates making the case for getting these interventions covered by insurance, the cost savings realized in the long run in early interventions was documented through an economics approach72. Early intervention, not surprisingly, costs more in the beginning in terms of added services, but eventually more than makes up for those upfront costs through savings in fewer services needed in adolescence and adulthood72.
In the past, many intervention and treatment studies have met with difficulties because accurate measures to study change over time in people with autism have not been developed or validated. In order to address this challenge, new measures have been designed and tested. One uses biosensors to collect biological data including heart rate, eye tracking and a sleep monitor, which will be used in future clinical trials to incorporate biological markers into treatment outcome73. Another used a portal EEG machine to track brain activity during a variety of circumstances and settings74. Importantly, two new behavioral instruments incorporating parental feedback into the final product were validated this year. The first was the direct result of the Patient Centered Outcome Research Institute, funded by the Affordable Care Act. This measure asks parents to nominate their top concerns for later tracking of treatment response. This measure has been shown to be valid in tracking symptoms of ADHD in children with autism75. The other, the Autism Family Experience Questionnaire (AFEQ), was developed with consistent input of parent groups and consists of four domains relating to parental perspectives, child social functioning, family life and child symptoms76.
How Technologies Can Enhance Interventions

Credit: Tim Reckmann
Technology has also shown to be an important adjunct to intervention protocols. For example, the smartglass (previously known as Google Glass) has been repurposed by other companies and has been shown to be well tolerated and fun for both children and adults with autism77,78, reducing symptoms of ASD, such as challenging behaviors, and improving non-verbal communication77. Augmentative and alternative communication (AAC) devices have also been studied in a variety of settings over the past few years, but surprisingly, they have only been investigated for a limited range of communicative gestures, like requesting79,80. Now, they are being studied and proving helpful in conjunction with, rather than replacing, naturalistic behavioral interventions81. Further research should focus on using these devices for a wider range of communication skills.
iPads, which are used by so many families or individuals with autism, were not previously studied scientifically in terms of their use for different purposes. In a new study this year, however, a group examined if the iPad was really helpful in enhancing the effectiveness of a home-based parent-delivered intervention. In fact, use of the iPad led to short-term improvements in autism-related behaviors and an increase in certain skills; however, the amount of time kids used the iPad in conjunction with the intervention declined over time82. They were probably still using the device, but not for its intended use. Newer applications will need to provide additional ways to engage users for the purpose of intervention. Other therapies, such as music therapy, were shown in a randomized trial to be no better than other therapies for core autism symptoms83. However, if you or your family love music, don’t drop music therapy yet – there is no evidence to say it is harmful or doesn’t work as an adjunct to more proven intervention techniques. Many parents I know who use music therapy use it in conjunction with other techniques.
More Findings About Females, But Much More Is Needed
In 2015, this summary was titled “The Year of the Female” due to the increase in studies focused on females with autism. This year saw a continued explosion in the knowledge around females with autism and how sex differences in those without autism can help inform why females have different symptoms and different prevalence of ASD. In fact, an entire issue of the journal Autism was devoted to scientific investigations of females with ASD84. The topics of this issue ranged from impressions from clinicians and psychometrics of current assessment instruments in females to why the prevalence of autism is different in males compared to females. This last question has intrigued and frustrated researchers, because understanding this difference might lead to a better understanding of the causes, treatment and measurement of both males and females with ASD.
What Explains the Gender Gap?
While previously assumed to be 4:1, the M:F bias in autism might actually be less. A new review and meta-analysis of millions of people shows variability across studies and calls into questions the original 4:1 number85. However, even at 3:1, there is a considerable difference in prevalence in autism between males and females, and several theories about what’s behind this disparity.
One theory is that females, through better innate social communication abilities, are able to camouflage their symptoms and mask their diagnosis. This has been observed in the naturalistic setting of recess in elementary schools, illustrated by females showing compensatory behaviors in social situations86. Camouflaging was also operationalized by a research group who defined it as the difference between how someone feels on the inside (self-report measures of autism symptoms and measures of social cognition) compared to how they appear on the outside (observational measures)87. Using this methodology revealed higher camouflaging scores in females87, further reinforcing this as a potential mechanism for diagnostic disparity. Unfortunately, higher camouflage scores were also associated with higher markers of depression, indicating the need to recognize psychiatric issues in females with ASD.

Another hypothesis for the difference in prevalence is that females are protected against an autism diagnosis. This year, additional evidence was published that supports the concept of a female protective effect in autism. This protective effect may be seen in the siblings of autistic females. To examine this using the big data approach, the rate of autism diagnosis in families was examined when the first child was a male vs. the first child was a female. When the older sibling was a female, recurrence rate was 1.3x higher than if the older sibling was a male88. This is consistent with other data finding that autistic females have more genetic mutations that are also seen in family members, but don’t always translate to an ASD diagnosis—hence, a protective effect in females with this shared genetic burden.
The female protective effect was also observed with regards to prenatal androgen levels. In children whose older sibling was a male, there was no association between cord blood levels of androgen and either early autism scores or social responsiveness. However, if the older sibling was a female, there was a positive association between prenatal testosterone and autism at both 12 and 36 months89. This could mean that the shared genetic liability seen in siblings of females changes sensitivity to prenatal androgen exposure. Finally, the protective effect was observed in brain tissue of individuals with autism. Female brains showed more dysregulated RNA levels, particularly in immune system and nervous system pathways, demonstrating a greater genetic load in females despite a lower prevalence90, consistent with other studies examining the differences in gene expression in males and females with ASD.
Let’s Talk About Sex
Possibly due in part from pressure from the self-advocacy community for more and higher quality research to help and better understand adults with autism, more scientific findings were published relating to the specific challenges faced by adults with ASD.
First, most diagnostic tools have traditionally been geared towards children with ASD. A new instrument called the 3Di-Adult takes about 40 minutes to administer and was shown to be both sensitive and specific91 to diagnosing autism in adults, providing a resource for adults who previously had not received a formal diagnosis.
Studies focused on sexuality in people with autism almost tripled this year, and many of them reinforced what the Neuroqueer movement has been saying for a while: People with autism are less likely to affiliate with an established gender or sexual orientation92-95. Autistic females are more likely to have more sexual partners, but also more negative sexual experiences compared to males93. A new sexual education program was released that has shown to help with what might be the biggest issue in sexuality in autistic adolescents and adults: poor or incomplete sexual education96.
Autism and Employment Challenges
Another important issue affecting many autistic adults is employment. After 10 years of gathering data from vocational rehabilitation services, it appears that the only predictor of employment outcome is number, not type, of VR services, suggesting “the more the better97”. Outside VR services, other factors predicted successful sustained employment. These included better independent living skills, receiving an inclusive education, and living in an urban environment (probably due to transportation issues)98. The good news is that the research community is paying special attention to employment issues, supporting a policy brief for employment, and developing new types of programs.
Big Findings Come From Big Data
This was another exciting year for autism research, using big data to better understand and isolate the factors that make people with autism similar and different. Whether you are a person with autism, a family member, a service provider, or someone else affected by autism—regardless of whether you agree on the needs of people with autism, no matter the IQ or verbal ability of you or your child—progress is being made each year to make your life better.
While it may be difficult to see in the very short term, giant gains continue to be made thanks to scientific advances that can be seen after 5 years, or even a decade. It’s frustrating to be told to “just be patient,” but the “informed hope” we should all have is that science and research will continue to provide answers—answers that help everyone.
Thank You

The research and the progress in care thanks to scientific understanding of autism does not happen without families and individuals who give their time and effort for these studies. Thank you! Researchers also play an important role—it’s not an especially glamorous job and the hourly pay would be way below minimum wage. The contributions by the entire autism community make these things possible. Want to participate? Register for the Autism BrainNet at www.takesbrains.org. Answer a few questions and spit into a tube and you can become part of Spark at www.sparkforautism.org. Spark is exactly the sort of “big data” project that will help understanding of individuals across the spectrum and what makes them so different.
References:
-
- (IACC) IACC. 016-2017 Interagency Autism Coordinating Committee Strategic Plan For Autism Spectrum Disorder. October 2017. : https://iacc.hhs.gov/publications/strategic-plan/2017/.2017.
- Pellicano E, Dinsmore A, Charman T. Views on researcher-community engagement in autism research in the United Kingdom: a mixed-methods study. PLoS One. 2014;9(10):e109946.
- Pellicano E, Dinsmore A, Charman T. What should autism research focus upon? Community views and priorities from the United Kingdom. Autism. 2014;18(7):756-770.
- Frazier T. The results are in: Priorities in autism research. 2017; https://www.autismspeaks.org/science/science-news/results-are-priorities-autism-research.
- Robison JE. Sex Lies and Autism Research – Getting Value for Our Money. 2017; https://www.psychologytoday.com/blog/my-life-aspergers/201711/sex-lies-and-autism-research-getting-value-our-money.
- Escher J. The Autism Matrix: A More Realistic Approach to Understanding the “Autisms”. 2017; https://www.sfautismsociety.org/blog/the-autism-matrix-a-more-realistic-approach-to-understanding-the-autisms.
- Fletcher-Watson S, Larsen K, Salomone E, Members of the CEWG. What do parents of children with autism expect from participation in research? A community survey about early autism studies. Autism. 2017:1362361317728436.
- Baron-Cohen S. Editorial Perspective: Neurodiversity – a revolutionary concept for autism and psychiatry. J Child Psychol Psychiatry. 2017;58(6):744-747.
- Tiura M, Kim J, Detmers D, Baldi H. Predictors of longitudinal ABA treatment outcomes for children with autism: A growth curve analysis. Res Dev Disabil. 2017;70:185-197.
- Solomon M, Iosif AM, Reinhardt VP, et al. What will my child’s future hold? phenotypes of intellectual development in 2-8-year-olds with autism spectrum disorder. Autism Res. 2017.
- Kim SH, Bal VH, Lord C. Longitudinal follow-up of academic achievement in children with autism from age 2 to 18. J Child Psychol Psychiatry. 2017.
- Visser JC, Rommelse NNJ, Lappenschaar M, Servatius-Oosterling IJ, Greven CU, Buitelaar JK. Variation in the Early Trajectories of Autism Symptoms Is Related to the Development of Language, Cognition, and Behavior Problems. J Am Acad Child Adolesc Psychiatry. 2017;56(8):659-668.
- Barbaro J, Dissanayake C. Diagnostic stability of autism spectrum disorder in toddlers prospectively identified in a community-based setting: Behavioural characteristics and predictors of change over time. Autism. 2017;21(7):830-840.
- Pathak M, Bennett A, Shui AM. Correlates of adaptive behavior profiles in a large cohort of children with autism: The autism speaks Autism Treatment Network registry data. Autism. 2017:1362361317733113.
- Kraper CK, Kenworthy L, Popal H, Martin A, Wallace GL. The Gap Between Adaptive Behavior and Intelligence in Autism Persists into Young Adulthood and is Linked to Psychiatric Co-morbidities. J Autism Dev Disord. 2017;47(10):3007-3017.
- Sparrow SS, Cicchetti, D.V., and Saulnier, C.A. . The Vineland Adaptive Behavior Scales, Third Edition. Bloomington, MN: NCS Pearson; 2016.
- Wittke K, Mastergeorge AM, Ozonoff S, Rogers SJ, Naigles LR. Grammatical Language Impairment in Autism Spectrum Disorder: Exploring Language Phenotypes Beyond Standardized Testing. Front Psychol. 2017;8:532.
- Wiggins LD, Tian LH, Levy SE, et al. Homogeneous Subgroups of Young Children with Autism Improve Phenotypic Characterization in the Study to Explore Early Development. J Autism Dev Disord. 2017;47(11):3634-3645.
- Mazurek MO, Lu F, Symecko H, et al. A Prospective Study of the Concordance of DSM-IV and DSM-5 Diagnostic Criteria for Autism Spectrum Disorder. J Autism Dev Disord. 2017.
- Grzadzinski R, Lord C, Sanders SJ, Werling D, Bal VH. Children with autism spectrum disorder who improve with fever: Insights from the Simons Simplex Collection. Autism Res. 2017.
- Weiner DJ, Wigdor EM, Ripke S, et al. Polygenic transmission disequilibrium confirms that common and rare variation act additively to create risk for autism spectrum disorders. Nat Genet. 2017;49(7):978-985.
- Turner TN, Coe BP, Dickel DE, et al. Genomic Patterns of De Novo Mutation in Simplex Autism. Cell. 2017;171(3):710-722 e712.
- Bishop SL, Farmer C, Bal V, et al. Identification of Developmental and Behavioral Markers Associated With Genetic Abnormalities in Autism Spectrum Disorder. Am J Psychiatry. 2017;174(6):576-585.
- Hudac CM, Stessman HAF, DesChamps TD, et al. Exploring the heterogeneity of neural social indices for genetically distinct etiologies of autism. J Neurodev Disord. 2017;9:24.
- Arnett AB, Cairney BE, Wallace AS, et al. Comorbid symptoms of inattention, autism, and executive cognition in youth with putative genetic risk. J Child Psychol Psychiatry. 2017.
- Tylee DS, Hess JL, Quinn TP, et al. Blood transcriptomic comparison of individuals with and without autism spectrum disorder: A combined-samples mega-analysis. Am J Med Genet B Neuropsychiatr Genet. 2017;174(3):181-201.
- van Rooij D, Anagnostou E, Arango C, et al. Cortical and Subcortical Brain Morphometry Differences Between Patients With Autism Spectrum Disorder and Healthy Individuals Across the Lifespan: Results From the ENIGMA ASD Working Group. Am J Psychiatry. 2017:appiajp201717010100.
- RK CY, Merico D, Bookman M, et al. Whole genome sequencing resource identifies 18 new candidate genes for autism spectrum disorder. Nat Neurosci. 2017;20(4):602-611.
- Lim ET, Uddin M, De Rubeis S, et al. Rates, distribution and implications of postzygotic mosaic mutations in autism spectrum disorder. Nat Neurosci. 2017;20(9):1217-1224.
- Krupp DR, Barnard RA, Duffourd Y, et al. Exonic Mosaic Mutations Contribute Risk for Autism Spectrum Disorder. Am J Hum Genet. 2017;101(3):369-390.
- Constantino JN, Kennon-McGill S, Weichselbaum C, et al. Infant viewing of social scenes is under genetic control and is atypical in autism. Nature. 2017;547(7663):340-344.
- Autism Spectrum Disorders Working Group of The Psychiatric Genomics C. Meta-analysis of GWAS of over 16,000 individuals with autism spectrum disorder highlights a novel locus at 10q24.32 and a significant overlap with schizophrenia. Mol Autism. 2017;8:21.
- St Pourcain B, Eaves LJ, Ring SM, et al. Developmental Changes Within the Genetic Architecture of Social Communication Behavior: A Multivariate Study of Genetic Variance in Unrelated Individuals. Biol Psychiatry. 2017.
- Ben-Shalom R, Keeshen CM, Berrios KN, An JY, Sanders SJ, Bender KJ. Opposing Effects on NaV1.2 Function Underlie Differences Between SCN2A Variants Observed in Individuals With Autism Spectrum Disorder or Infantile Seizures. Biol Psychiatry. 2017;82(3):224-232.
- Escamilla CO, Filonova I, Walker AK, et al. Kctd13 deletion reduces synaptic transmission via increased RhoA. Nature. 2017;551(7679):227-231.
- Stoodley CJ, D’Mello AM, Ellegood J, et al. Altered cerebellar connectivity in autism and cerebellar-mediated rescue of autism-related behaviors in mice. Nature Neuroscience. 2017;20(12):1744-1751.
- Raghavan R, Riley AW, Volk H, et al. Maternal Multivitamin Intake, Plasma Folate and Vitamin B12 Levels and Autism Spectrum Disorder Risk in Offspring. Paediatr Perinat Epidemiol. 2017.
- DeVilbiss EA, Magnusson C, Gardner RM, et al. Antenatal nutritional supplementation and autism spectrum disorders in the Stockholm youth cohort: population based cohort study. BMJ. 2017;359:j4273.
- Wang M, Li K, Zhao D, Li L. The association between maternal use of folic acid supplements during pregnancy and risk of autism spectrum disorders in children: a meta-analysis. Mol Autism. 2017;8:51.
- Goodrich AJ, Volk HE, Tancredi DJ, et al. Joint effects of prenatal air pollutant exposure and maternal folic acid supplementation on risk of autism spectrum disorder. Autism Res. 2017.
- Kim D, Volk H, Girirajan S, et al. The joint effect of air pollution exposure and copy number variation on risk for autism. Autism Res. 2017;10(9):1470-1480.
- Webb SJ, Garrison MM, Bernier R, McClintic AM, King BH, Mourad PD. Severity of ASD symptoms and their correlation with the presence of copy number variations and exposure to first trimester ultrasound. Autism Res. 2017;10(3):472-484.
- Ackerman S, Schoenbrun S, Hudac C, Bernier R. Interactive Effects of Prenatal Antidepressant Exposure and Likely Gene Disrupting Mutations on the Severity of Autism Spectrum Disorder. J Autism Dev Disord. 2017;47(11):3489-3496.
- Spann MN, Sourander A, Surcel HM, Hinkka-Yli-Salomaki S, Brown AS. Prenatal toxoplasmosis antibody and childhood autism. Autism Res. 2017;10(5):769-777.
- Mahic M, Mjaaland S, Bovelstad HM, et al. Maternal Immunoreactivity to Herpes Simplex Virus 2 and Risk of Autism Spectrum Disorder in Male Offspring. mSphere. 2017;2(1).
- Pardo CA, Farmer CA, Thurm A, et al. Serum and cerebrospinal fluid immune mediators in children with autistic disorder: a longitudinal study. Mol Autism. 2017;8:1.
- Lombardo MV, Moon HM, Su J, Palmer TD, Courchesne E, Pramparo T. Maternal immune activation dysregulation of the fetal brain transcriptome and relevance to the pathophysiology of autism spectrum disorder. Mol Psychiatry. 2017.
- Hornig M, Bresnahan MA, Che X, et al. Prenatal fever and autism risk. Mol Psychiatry. 2017.
- Schieve LA, Tian LH, Drews-Botsch C, et al. Autism spectrum disorder and birth spacing: Findings from the study to explore early development (SEED). Autism Res. 2017.
- Oberlander TF, Zwaigenbaum L. Disentangling Maternal Depression and Antidepressant Use During Pregnancy as Risks for Autism in Children. JAMA. 2017;317(15):1533-1534.
- Schieve LA, Drews-Botsch C, Harris S, et al. Maternal and Paternal Infertility Disorders and Treatments and Autism Spectrum Disorder: Findings from the Study to Explore Early Development. J Autism Dev Disord. 2017;47(12):3994-4005.
- Singer AB, Burstyn I, Thygesen M, Mortensen PB, Fallin MD, Schendel DE. Parental exposures to occupational asthmagens and risk of autism spectrum disorder in a Danish population-based case-control study. Environ Health. 2017;16(1):31.
- Janecka M, Rijsdijk F, Rai D, Modabbernia A, Reichenberg A. Advantageous developmental outcomes of advancing paternal age. Transl Psychiatry. 2017;7(6):e1156.
- Golding J, Ellis G, Gregory S, et al. Grand-maternal smoking in pregnancy and grandchild’s autistic traits and diagnosed autism. Sci Rep. 2017;7:46179.
- Dunaway KW, Islam MS, Coulson RL, et al. Cumulative Impact of Polychlorinated Biphenyl and Large Chromosomal Duplications on DNA Methylation, Chromatin, and Expression of Autism Candidate Genes. Cell Rep. 2016;17(11):3035-3048.
- Ellis SE, Gupta S, Moes A, West AB, Arking DE. Exaggerated CpH methylation in the autism-affected brain. Mol Autism. 2017;8:6.
- Nardone S, Sams DS, Zito A, Reuveni E, Elliott E. Dysregulation of Cortical Neuron DNA Methylation Profile in Autism Spectrum Disorder. Cereb Cortex. 2017;27(12):5739-5754.
- Weir RK, Bauman MD, Jacobs B, Schumann CM. Protracted dendritic growth in the typically developing human amygdala and increased spine density in young ASD brains. J Comp Neurol. 2017.
- Hashemi E, Ariza J, Rogers H, Noctor SC, Martinez-Cerdeno V. The Number of Parvalbumin-Expressing Interneurons Is Decreased in the Prefrontal Cortex in Autism. Cereb Cortex. 2017:1.
- Adorjan I, Ahmed B, Feher V, et al. Calretinin interneuron density in the caudate nucleus is lower in autism spectrum disorder. Brain. 2017;140(7):2028-2040.
- Wegiel J, Flory M, Kaczmarski W, et al. Partial Agenesis and Hypoplasia of the Corpus Callosum in Idiopathic Autism. J Neuropathol Exp Neurol. 2017;76(3):225-237.
- Hazlett HC, Gu H, Munsell BC, et al. Early brain development in infants at high risk for autism spectrum disorder. Nature. 2017;542(7641):348-351.
- Emerson RW, Adams C, Nishino T, et al. Functional neuroimaging of high-risk 6-month-old infants predicts a diagnosis of autism at 24 months of age. Sci Transl Med. 2017;9(393).
- Eggebrecht AT, Elison JT, Feczko E, et al. Joint Attention and Brain Functional Connectivity in Infants and Toddlers. Cereb Cortex. 2017;27(3):1709-1720.
- Wolff JJ, Swanson MR, Elison JT, et al. Neural circuitry at age 6 months associated with later repetitive behavior and sensory responsiveness in autism. Mol Autism. 2017;8:8.
- Shen MD, Kim SH, McKinstry RC, et al. Increased Extra-axial Cerebrospinal Fluid in High-Risk Infants Who Later Develop Autism. Biol Psychiatry. 2017;82(3):186-193.
- Levin AR, Varcin KJ, O’Leary HM, Tager-Flusberg H, Nelson CA. EEG power at 3 months in infants at high familial risk for autism. J Neurodev Disord. 2017;9(1):34.
- Bedford R, Gliga T, Shephard E, et al. Neurocognitive and observational markers: prediction of autism spectrum disorder from infancy to mid-childhood. Mol Autism. 2017;8:49.
- Damiano-Goodwin CR, Woynaroski TG, Simon DM, et al. Developmental sequelae and neurophysiologic substrates of sensory seeking in infant siblings of children with autism spectrum disorder. Dev Cogn Neurosci. 2017.
- Miller M, Iosif AM, Hill M, Young GS, Schwichtenberg AJ, Ozonoff S. Response to Name in Infants Developing Autism Spectrum Disorder: A Prospective Study. J Pediatr. 2017;183:141-146 e141.
- Green J, Pickles A, Pasco G, et al. Randomised trial of a parent-mediated intervention for infants at high risk for autism: longitudinal outcomes to age 3 years. J Child Psychol Psychiatry. 2017;58(12):1330-1340.
- Cidav Z, Munson J, Estes A, Dawson G, Rogers S, Mandell D. Cost Offset Associated With Early Start Denver Model for Children With Autism. J Am Acad Child Adolesc Psychiatry. 2017;56(9):777-783.
- Ness SL, Manyakov NV, Bangerter A, et al. JAKE(R) Multimodal Data Capture System: Insights from an Observational Study of Autism Spectrum Disorder. Front Neurosci. 2017;11:517.
- Billeci L, Tonacci A, Tartarisco G, et al. An Integrated Approach for the Monitoring of Brain and Autonomic Response of Children with Autism Spectrum Disorders during Treatment by Wearable Technologies. Front Neurosci. 2016;10:276.
- Scahill L, Bearss K, Sarhangian R, et al. Using a Patient-Centered Outcome Measure to Test Methylphenidate Versus Placebo in Children with Autism Spectrum Disorder. J Child Adolesc Psychopharmacol. 2017;27(2):125-131.
- Leadbitter K, Aldred C, McConachie H, et al. The Autism Family Experience Questionnaire (AFEQ): An Ecologically-Valid, Parent-Nominated Measure of Family Experience, Quality of Life and Prioritised Outcomes for Early Intervention. J Autism Dev Disord. 2017.
- Liu R, Salisbury JP, Vahabzadeh A, Sahin NT. Feasibility of an Autism-Focused Augmented Reality Smartglasses System for Social Communication and Behavioral Coaching. Front Pediatr. 2017;5:145.
- Keshav NU, Salisbury JP, Vahabzadeh A, Sahin NT. Social Communication Coaching Smartglasses: Well Tolerated in a Diverse Sample of Children and Adults With Autism. JMIR Mhealth Uhealth. 2017;5(9):e140.
- Holyfield C, Drager KDR, Kremkow JMD, Light J. Systematic review of AAC intervention research for adolescents and adults with autism spectrum disorder. Augment Altern Commun. 2017;33(4):201-212.
- Logan K, Iacono T, Trembath D. A systematic review of research into aided AAC to increase social-communication functions in children with autism spectrum disorder. Augment Altern Commun. 2017;33(1):51-64.
- Chang YC, Shih W, Landa R, Kaiser A, Kasari C. Symbolic Play in School-Aged Minimally Verbal Children with Autism Spectrum Disorder. J Autism Dev Disord. 2017.
- Whitehouse AJO, Granich J, Alvares G, et al. A randomised controlled trial of an iPad-based application to complement early behavioural intervention in Autism Spectrum Disorder. J Child Psychol Psychiatry. 2017;58(9):1042-1052.
- Crawford MJ, Gold C, Odell-Miller H, et al. International multicentre randomised controlled trial of improvisational music therapy for children with autism spectrum disorder: TIME-A study. Health Technol Assess. 2017;21(59):1-40.
- Mandy W, Lai MC. Towards sex- and gender-informed autism research. Autism. 2017;21(6):643-645.
- Loomes R, Hull L, Mandy WPL. What Is the Male-to-Female Ratio in Autism Spectrum Disorder? A Systematic Review and Meta-Analysis. J Am Acad Child Adolesc Psychiatry. 2017;56(6):466-474.
- Dean M, Harwood R, Kasari C. The art of camouflage: Gender differences in the social behaviors of girls and boys with autism spectrum disorder. Autism. 2017;21(6):678-689.
- Lai MC, Lombardo MV, Ruigrok AN, et al. Quantifying and exploring camouflaging in men and women with autism. Autism. 2017;21(6):690-702.
- Palmer N, Beam A, Agniel D, et al. Association of Sex With Recurrence of Autism Spectrum Disorder Among Siblings. JAMA Pediatr. 2017;171(11):1107-1112.
- Park BY, Lee BK, Burstyn I, et al. Umbilical cord blood androgen levels and ASD-related phenotypes at 12 and 36 months in an enriched risk cohort study. Mol Autism. 2017;8:3.
- Schumann CM, Sharp FR, Ander BP, Stamova B. Possible sexually dimorphic role of miRNA and other sncRNA in ASD brain. Mol Autism. 2017;8:4.
- Mandy W, Clarke K, McKenner M, et al. Assessing Autism in Adults: An Evaluation of the Developmental, Dimensional and Diagnostic Interview-Adult Version (3Di-Adult). J Autism Dev Disord. 2017.
- George R, Stokes MA. Sexual Orientation in Autism Spectrum Disorder. Autism Res. 2017.
- Hancock GIP, Stokes MA, Mesibov GB. Socio-sexual functioning in autism spectrum disorder: A systematic review and meta-analyses of existing literature. Autism Res. 2017;10(11):1823-1833.
- Turner D, Briken P, Schottle D. Autism-spectrum disorders in adolescence and adulthood: focus on sexuality. Curr Opin Psychiatry. 2017;30(6):409-416.
- May T, Pang KC, Williams K. Brief Report: Sexual Attraction and Relationships in Adolescents with Autism. J Autism Dev Disord. 2017;47(6):1910-1916.
- Dekker LP, van der Vegt EJM, van der Ende J, et al. Psychosexual Functioning of Cognitively-able Adolescents with Autism Spectrum Disorder Compared to Typically Developing Peers: The Development and Testing of the Teen Transition Inventory- a Self- and Parent Report Questionnaire on Psychosexual Functioning. J Autism Dev Disord. 2017;47(6):1716-1738.
- Alverson CY, Yamamoto SH. VR Employment Outcomes of Individuals with Autism Spectrum Disorders: A Decade in the Making. J Autism Dev Disord. 2017.
- Chan W, Smith LE, Hong J, Greenberg JS, Lounds Taylor J, Mailick MR. Factors associated with sustained community employment among adults with autism and co-occurring intellectual disability. Autism. 2017:1362361317703760.