

Year End Summary: 2019
By Alycia Halladay, PhD, Chief Science Officer and The Scientific Advisory Board of ASF
Listen to the 2019 Year End Summary here.
The ASF Yearly Summary of Science highlights major research accomplishments that directly affect the lives of families with autism spectrum disorder (ASD). These accomplishments impact families in a number of ways: by affording those diagnosed and their families a better understanding of a particular behavior or biological feature; identifying beneficial treatment targets, interventions, services or resources; discovering technologies that not only identify unique characteristics of people with ASD but also offer insight as to how to better serve that population and by offering future predictions.
ASD research continues to be challenged by clinical heterogeneity, a scientific term applied to the variability of symptoms found in subjects across the spectrum. Current research has identified increased diversity amongst people with autism participating in research; in turn, this has led to a reduction across time in differences between people with a diagnosis vs. those without a diagnosis1. In other words, those participating in research now show less severe features of ASD compared to 20 years ago. This reflects the inclusion of a more diverse set of people with autism, however, those on the more profoundly affected end may not see the benefits of research that predominantly includes those with completely different features of ASD. One solution proffered to rectify this challenge has been to stratify individuals with ASD into different groups for the purposes of research. Although advocates report that stratification lends itself to precisely determining the needs of specific groups and individuals, other researchers continue to cluster individuals into one group. Whether to stratify or cluster is a prominent discussion amongst scientists and advocates and could become polarizing, as both approaches affect research, basic nomenclature, services such as housing and employment and support services.

- Features in infancy predict adult outcomes
Multiple studies this year have linked children’s symptoms and biology in infancy to later outcomes. Motor abilities, family history, brain connectivity all can independently contribute to how a child develops over time. These outcomes include an autism diagnosis, verbal ability, and cognition in adulthood. This sort of research can be used to help prepare families and customize interventions that focus on the most debilitating symptoms of ASD.
This year, to make predictions about future ASD features, more studies used a longitudinal study design. This design is critical to autism research because it follows a group comprised of individuals diagnosed with ASD and, at times, individuals without a diagnosis in order to determine how they are affected as adolescents and adults. Whereas a longitudinal study can be expensive, complex and does not produce immediate results, the nature of its design provides clinicians invaluable data, affording deeper insights that allow them to more fully educate families by managing expectations, identifying focus areas and providing coping strategies that serve to help those with ASD live their best lives.
Longitudinal studies help parents understand their child’s reality and manage future expectations, as well as help scientists refine interventions according to the variability of groups of people with ASD. Multiple research studies have used data to group children based on trajectory, i.e. the progression from commencement, through adolescent development to adult functioning. The composition of these groups consists of those who show fewer symptoms and continue to improve vs. those less functioning who continue to decline. This year, two longitudinal studies, one conducted in the United States and one in Canada, closely examined toddlers to pinpoint and study specific factors that influence outcomes, from childhood to adulthood. In these studies, two patterns emerged: those possessing lower levels of symptoms who improve vs. those with more profound symptoms who decline.
While all groups showed improvement in daily living skills, those who presented less severe symptoms in toddlerhood and showed marked progression during adolescence also had the highest adaptive abilities as adults2. Although most participants showed improvement in social communication with age, improvement varied, based on individual language ability as toddlers. Social communication impairments in 19 year olds was found to correlate with differences in language ability as early as age two. As speech improved, so did this core symptom of ASD3: those with early minimal language ability showed the greatest functioning impairments as adults. Likewise, fine motor skills in infancy4 is a predictor of language at age 19, in that better fine motor skills in early childhood is a predictor of better command of language in adulthood. Together, these findings demonstrate that poor early motor skills and decreased language function are related to later ASD symptoms. This is a crucial identification, considering that both fine motor skills and language are target areas of early intervention and that intervention may improve ASD through adulthood.
The study of early motor function is not only vital to further understanding how it affects those diagnosed, it also offers insight pre-diagnosis in terms of how early motor function may predict a later ASD diagnosis. The Baby Siblings Research Consortium (BSRC) is a group of researchers that studies initial features of ASD in siblings of children with ASD as young as 6 weeks of age. Siblings of children with ASD have a 15x greater probability of having ASD themselves than do other children. Similar to previously mentioned studies, BSRC also concludes that fine motor abilities at 6 months can predict an ASD diagnosis in siblings and expressive language ability in younger siblings at 3 years6,7.
Another factor BSRC researchers have employed to estimate the probability of diagnosis in children is number of siblings previously diagnosed with ASD. Those with at least 2 older siblings with ASD were found to have a higher probability of a diagnosis, as well as increased severe cognitive disabilities8. Based on family history, this information is vital in helping families better understand the probability of an ASD diagnosis in future children, as well as predicting strengths and limitations future children may face.
In addition to identifying behavioral markers, the past decade of research has revealed a blossoming of early biological factors that may serve as additional predictors of diagnosis, ranging from genetic tests9, salivary hormone markers and other reflections of altered development. Studies of brain structure, activity and connectivity have also proven valuable; when measured non-invasively, identified changes in activity in the frontal lobe of the brain during the first year of life have served to predict an ASD diagnosis in infant siblings10. Because brain wavelengths vary, identifying and monitoring changes in the size of each different type of wavelength over the course of a year serves as valuable information in terms of not just determining an ASD diagnosis but also for further understanding brain fluctuations during that time period10.
Complementary to brain activity, previous studies from the Infant Brain Imaging Network (IBIS) revealed different approaches to more accurately predicting ASD diagnosis by using measurements of brain structure and connectivity, in addition to mathematical algorithms based on the shape and function of different brain regions, as potential predictors of a later diagnosis. This year, the analysis of early brain based ASD markers has afforded scientists more precision in determining an association with brain connectivity in critical ASD brain regions, as well as an insistence on sameness and stereotyped behaviors at 12 – 24 months11. Not only do these biological based markers aide in predicting later diagnosis and identifying features of ASD within a diagnosis, they have the potential to serve as objective ways to help determine specific interventions, both medical and behavioral.

2. Screening is not perfect, but it is essential
New technologies contribute to greater use of standardized measures in different community settings. At the same time, clinicians and scientists have developed new ways to use common records and tools, resulting in better identification of concerns at even earlier stages. Families and care providers should confidently screen early and often.
Biological based markers hold promise for even earlier detection of features, especially in those with a family history. However, to make predictions about not just a diagnosis but future expectations of needs as well, most care providers, physicians and clinicians rely on behavioral concerns. Right now, most families lack access to EEG machines and MRIs and expensive genetic testing is most often not covered by insurance. The reality of early detection of ASD in 2019 is that it occurs mostly in primary care settings, where physicians help to interpret results for the family. In 2019, the AAP published an update to their 2007 guidelines for screening for autism and it continues to recommend autism-specific screening at 18 and 24 months12. Researchers continue to explore new ways to make this tool more accessible via technology, such as electronic tablets, whereas scientists continue to refine and improve accuracy screening tools using machine learning13.
One challenge of current screening practices (and in fact, in all of ASD research) is the disparity in screening and screening results amongst distinct racial and ethnic groups14. In order to address these differences, scientists are analyzing a variety of approaches fashioned to deal with these disparities and to increase access to screening tools. This includes remotely employing video based tools to capture ASD features to help identify and diagnosis ASD15-17. These video based tools help parents identify signs by providing real life examples of parent-child interactions18 and by examining existing reports of developmental milestones from electronic medical records19, with the goal of identifying early signs of developmental concerns as soon as possible, in as many infants as possible, regardless of race or ethnicity . Doing so will increase early diagnosis, leading to earlier intervention and increased understanding of ASD, self-awareness of symptoms and long-term improvement of services.
3. The lifespan of mental health challenges sparks new intervention possibilities
The high rate of mental health disorders in both children and adults with ASD means that a large percentage of this population and their families are burdened with enormous challenges Training community providers to deliver mental health interventions shows promise for alleviating these comorbidities. Clinicians need to be on the lookout for these psychiatric issues so people with autism receive the much-needed services they deserve.
While the core symptoms of ASD often lead to challenges in daily functioning, across the lifetime and spectrum of many individuals with ASD, co-occurring mental health conditions are a huge concern. Several older but smaller international studies provide a wide range of estimates of the prevalence of co-occurring conditions. A met- analysis and systematic review of these studies conducted in 2019 has helped to decipher the findings20. The findings revealed 28% comorbidity of ADHD (higher in kids than adults), 20% for anxiety disorders, 11% for depression and 9% for obsessive-compulsive disorder20. There is even overlap in brain based profiles of different diagnoses, both in terms of genetic activity21 and structure22. These mental health issues, particularly anxiety, can lead to an acute crisis requiring hospitalization23. Unfortunately, clinicians have limited knowledge and understanding of the nature of these mental health conditions in ASD24, making intervention difficult. However, ASD researchers have had luck training community mental health providers to deliver interventions focused on addressing these mental health challenges25. Training community based providers is a move in a promising direction, allowing more people to receive services in a variety of settings, but the efficacy of these interventions still lags behind those delivered in clinics26. Understanding the high co-occurrence of mental health issues helps families and individuals both plan for later health care needs and anticipate potential mental health problems before they occur.
4. Heritable factors that influence brain development result in multiple psychiatric conditions, including autism.
Researchers have determined that of the over 100 autism genes that exist, all act on early developmental functions and lead to diverse, overlapping outcomes, including psychiatric disorders, autism, and related conditions. Some genetic influences, while rare, can help define the mechanisms that lead to brain cells in autism developing over time. Although a link has been established connecting environmental influences to this same spectrum of conditions, few studies have successfully defined their interaction. These findings have implications for interventions and could lead to strategies for mitigating symptoms.
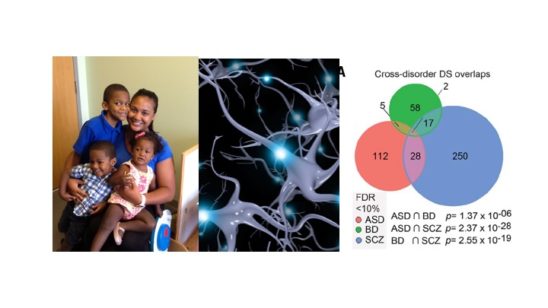
Given the comorbidity of mental health disorders with autism spectrum disorder, it should come as no surprise that new research reveals that ASD relevant genes act in fundamental ways that may influence multiple outcomes, ranging from ASD to schizophrenia, to ADHD27-30, neurodevelopmental disorders and intellectual disability31-33. Genes that act on such early and fundamental brain pathways have downstream effects on a number of brain functions, ASD being one of them. This might explain why there are so many ASD genes and why they are pleiotropic, meaning they have different functions. In fact, the list of genes associated with ASD keeps growing, as larger studies and better technology have revealed over 150 ASD associated genes34. Infant siblings of children with autism also show rare and common gene variants in ASD genes that can aid in a diagnosis9.
In addition, the presence of certain genetic mutations in ASD relevant genes can produce profound disabilities, which alone work to explain an ASD diagnosis. These mutations, referred to as rare genetic variants, are important to the community because their discovery has led to the creation of Patient Advocacy Groups that provide support and resources for focused research, as well as offer pathways to better understanding the basic circuitry of certain ASD behaviors35. Scientists are studying these rare genetic forms of ASD to understand all forms of ASD, particularly gene expression in the brain36,37. When compared to studies of the brains of people with bipolar disorder and schizophrenia, studies of brain tissue in people with ASD reveal overlapping genetic activity in genes that control synaptic signaling, neurotransmitter release, and immune response.36,37. The abnormal immune signaling in the brain might result in cell damage, as evidenced by accumulation of T-cells in brain tissue38. Studying the brains of people with ASD is the best way to understand the basic cellular and molecular basis of ASD, and is only possible through families who decide at the most difficult time to make the decision to donate. If you would like to learn more about the Autism BrainNet, which made these studies possible, visit www.takesbrains.org/signup.
While genetic factors are incredibly important in the diagnosis and presentation of symptoms of ASD, understanding the role of environmental factors in both the diagnosis and presentation of symptoms of ASD is crucial. One of the most studied environmental factors in ASD is exposure to air pollution during pregnancy. This year, ancillary evidence taken from additional locations via different methodologies shows a particular effect for a component in air pollution called PM (particulate matter) 2.5 (2.5 microns)39. Air pollution exposure may interact with maternal diabetes, which also increases the probability of ASD40. Air pollution also seems to influence an ASD diagnosis more strongly in boys41. It is important that public health policy address established, scientifically based environmental factors to address even smaller, but preventable, environmental factors.
There have been spurious reports of other environmental factors, but rather than look at factors in isolation, it is crucial to understand how these factors collectively influence brain development and interact with genetic susceptibility, either rare genetic or polygenic influences36. Another area of convergence of environmental and genetic factors is epigenetics, often called the “second genome”. The epigenome is a multitude of chemicals and tags on the DNA genome that is responsive to environmental factors that can turn on or turn off DNA expression, as early as when the embryo is formed. ASD risk genes identified in genetic studies can also work epigenetically42-46. The next generation of research will hopefully focus on understanding the multifactorial influences of an ASD diagnosis, how these factors affect symptoms and influence long term trajectories across neuropsychiatric diagnoses, including ASD.

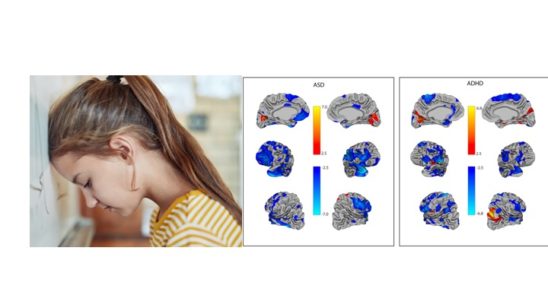
5. Females with autism present features differently
Females with autism show opposite neurobiological features of autism, while also possessing some of the same core features of ASD. In females, these differences may be found in the way symptoms present or in associated features of ASD. Lack of differentiation clouds important scientific discoveries, which is why treatments and services should be sex specific.
Over the past five years, ASD research has increasingly focused more attention on identifying and understanding how autism manifests in females; this includes, but is not limited, to: genetic makeup, symptom presentation, long term trajectory and mental health issues. Females are diagnosed 4x less often but also have an increased load of genetic mutations, including recessive mutations47. This year, results of studies have been mixed in terms of the magnitude and nature of sex and gender related symptom presentation in males vs. females, noting a problem plaguing ASD research mentioned earlier: heterogeneity48. Differences across sex and gender are not seen in terms of presence or absence of symptoms, but rather in the way they present across different ages49,50. On the whole, differences are few in infants and toddlers but are magnified during adolescence, even in the way people perceive ASD symptoms in males and females51. Some scientists suggest that associated symptoms are most likely to present differently than core symptoms of ASD52, with females showing a higher prevalence of ADHD53 and OCD, leading to differences in the way males and females appear.
In addition to findings of increased numbers of recessive mutations in the genome of females47, analysis of brain structure has revealed sex differences further suggestive of the female protective effect. Focused study of the cerebellum has revealed that female activation patterns oppose those of males with ASD 54 and fail to evince similar patterns of connectivity across different brain regions55,56, i.e. females with ASD show reduced connectivity compared to females without ASD, an effect not seen in males with ASD55. In addition, when comparing twins, females had more profound differences in the sizes of brain regions compared to males57. These findings have led researchers to refine how they examine the role gender plays in basic science research.
Animal model research suggests that environmental exposures may not produce the same impairments in male vs. female offspring58. Taken together, these biological findings demonstrate that females, despite demonstrating a lower prevalence of ASD, also show complicated behavioral features and more biological markers for ASD. Future research must focus on why females are diagnosed less often than males and why, when they are diagnosed, they present more behavioral markers than their male counterparts.

6. It takes a village to make interventions work in the classroom
Teachers play a considerable role in identifying and helping kids across the spectrum, which is why teachers need focused training and support in order to best serve students with ASD.
Teachers and school administrators must perform a multitude of duties and responsibilities in an effort to meet the needs of students of varying abilities within the same classroom and provide all students – those on the spectrum and those who are not – with an equal opportunity to learn. In a perfect world, each student in our school systems would receive exactly what he or she needs, when it is needed, regardless of school systems and across different symptom presentation. Unfortunately, in 2019, researchers documented that in some states, the diagnosis of ASD does not necessarily correspond to the educational classification59, an inconsistency which might create disparities in service utilization across states, particularly considering that the quality of programs in many school systems rate just above adequate60.
Adding to these challenges in schools, research shows that students with ASD who exhibit unclear symptom presentation are likely to receive different services61,62. Teacher perception of what is effective often dictates what kind of evidence-based interventions are used in the school system63. Therefore, the specific types of support services students need in order to be successful often do not match up to what they actually receive. Studying clinic-based interventions in real world settings, such as in schools, is challenging as well. The biggest problem is that these interventions don’t always translate fluidly from clinic to classroom26 and often require modifications just to get them into the classroom. For example, according to research, a popular curriculum called TeachTown, commonly used by classroom teachers, does not necessarily help kids with ASD64. The good news is scientists are using opportunities like recess65 for social interventions in ASD.
Of real concern is that the types of educational based interventions can vary based on ethnic group66, leading to inequity in services. While racial and ethnic disparities continue to exist, researchers are exploring different methods to alleviate these differences. While Medicaid waivers have been shown to be somewhat helpful67, most research so far has focused more on defining the problem, so that future studies can be set up to address these challenges directly. Transition to employment in the school system can be improved by the perspectives of those that have successes and challenges with employment. This includes starting early and help build environmental supports for future success on the job68. These findings will lead to more tailored and effective intervention strategies to improve services for all people across the spectrum in schools, where they are desperately needed.
7. Model systems of autism are used to understand the earliest, fundamental features of ASD.
Scientists use animals and cells to determine what happens at the onset of autism and when it happens, beginning with the moment the cells are formed, in order to better build interventions for different times in development.
Animals do not have ASD. Cells in a dish do not have ASD. But animals and cells can still provide important insight into not just therapeutic targets but can also offer a comprehensive understanding on what is happening in the brains and bodies of people with ASD. The cells in a dish actually come from cells in a person, including those with idiopathic and rare genetic forms of ASD. By using induced pluripotent stem cell (iPSC) technologies to transform a skin cell into a brain cell and then back into a skin cell, important discoveries about individual brain development can emerge. These models have revealed that certain genes cause neurons to be overconnected69 while others can impair the strengths of those connections70 or reduce neuronal activity on the cellular level71. These are the basic fundamental properties of cell development that seem to be common across multiple psychiatric conditions, including autism.
In turn, animal models allow for a more complex analysis of single genes in the presence of organisms with other genes. Together with findings in brain tissue, these animal models have shown that, despite the gene involved, there are converging networks that could be the target of future interventions72. Animal models can also demonstrate which gene x environment interactions exacerbate symptoms or alleviate symptoms in a controlled setting73,74. They have also been able to identify the underlying molecular mechanisms of genetic mutations associated with ASD75,76. Beyond the brain, these new models can identify mechanisms of associated dysfunction like gastrointestinal functions75 which plague many families with ASD. A new technology introduced last year called CRISPR allows researchers to better target genes one at a time or in combination to better understand the roles of genes as well as gene x environment interactions on basic functioning of cells across the body and what this means for humans, helping them both understand and anticipate specific symptoms across time.

8. While scientists now know more about interventions, there is much that they still need to learn.
While the efficacy of fluoxetine for repetitive behaviors has been addressed, other treatments such as fecal transplants, stem cell transplants and cannabidiol still lack an evidence base and therefore use is not recommended at this time. The autism community should be cautious of interventions that lack strong scientific research, as well as by wary of flashy headlines
This year, advances in behavioral interventions for ASD revealed a common theme: remote delivery. This includes development of telehealth methods77 and videoconferencing78. As mentioned earlier, this methodology will expand coverage while striving to ensure quality. However, findings also demonstrated what does not work. For example, fluoxetine, or Prozac, has proved to be ineffective for repetitive behaviors in ASD79,80 however that does not mean people should go off of their medication if it is helping them in other areas, but instead they should be aware that it may not help the core symptoms of ASD. On the other hand, new research in other drug targets, including the vasopressin receptor, showed promise in males81. While more work needs to be done, scientists have a better understanding of what works for particular symptoms in specific people.
Although much is known, there is a great need to acknowledge emerging fields where little is known, especially in the field of intervention. Media reports hyping the effectiveness of stem cell studies and fecal transplants pushed these alternative treatments into public view however, the designs were subject to bias82 or had small sample sizes83, suggesting further caution when considering these alternative, non-evidence based approaches. On the other hand, the target of the fecal transplants, the microbiome, has been understudied in basic and clinical studies. Probiotics have also led to improvements in gastrointestinal function in people with ASD85, providing evidence that the microbiome is important but needs further study, both in determining mechanism in model systems and more precise intervention therapies.
Another alternative therapy used by families with no substantial scientific evidence is medical marijuana, including the psychoactive component THC and a non-psychoactive chemical within the cannabis plant called CBD. Unfortunately, again, media hype and marketing strategies have provided hope where scientific evidence is lacking. Research in this area is hampered by legal and administrative policies, but newer, more definitive research studies are in progress. While there is reason to be hopeful in this area, there is also reason to be cautious. People with ASD respond differently to CBD than those without ASD86, and parents should not assume what works in one child without ASD will work in their child with ASD.
The Autism Science Foundation recognizes that there is much scientific information available from multiple sources that can be accessed on multiple platforms. This summary is meant to highlight this year’s advances, including differences that have changed over time and across sex, as well as shed light on similarities with other neuropsychiatric disorders. It is hard for anyone to make sense of it all when it is announced, or even as these discoveries build on each other. However, it’s important to know that advancements in understanding the basic biology of ASD have led to more specific interventions, increased knowledge of what works and what does work, further expansion in utility across settings and lastly, clues for future studies. Although this summary does not capture every insight and advancement revealed in scientific studies of ASD this year, ASF feels that these highlights offer a comprehensive overview and it will continue to share science news throughout 2020, particularly what is most valuable in helping family members understand how to best serve loved ones with ASD and themselves.
References:
1. Rodgaard EM, Jensen K, Vergnes JN, Soulieres I, Mottron L. Temporal Changes in Effect Sizes of Studies Comparing Individuals With and Without Autism: A Meta-analysis. JAMA Psychiatry. 2019.
2. Di Rezze B, Duku E, Szatmari P, et al. Examining Trajectories of Daily Living Skills over the Preschool Years for Children with Autism Spectrum Disorder. J Autism Dev Disord. 2019;49(11):4390-4399.
3. Bal VH, Kim SH, Fok M, Lord C. Autism spectrum disorder symptoms from ages 2 to 19 years: Implications for diagnosing adolescents and young adults. Autism Res. 2019;12(1):89-99.
4. Bal VH, Fok M, Lord C, et al. Predictors of longer-term development of expressive language in two independent longitudinal cohorts of language-delayed preschoolers with Autism Spectrum Disorder. J Child Psychol Psychiatry. 2019.
5. Cain MK, Kaboski JR, Gilger JW. Profiles and academic trajectories of cognitively gifted children with autism spectrum disorder. Autism. 2019;23(7):1663-1674.
6. Iverson JM, Shic F, Wall CA, et al. Early motor abilities in infants at heightened versus low risk for ASD: A Baby Siblings Research Consortium (BSRC) study. J Abnorm Psychol. 2019;128(1):69-80.
7. LeBarton ES, Landa RJ. Infant motor skills predicts later expressive language and autism spectrum disorder diagnosis. Infant Behav Dev. 2019;54:37-47.
8. McDonald NM, Senturk D, Scheffler A, et al. Developmental Trajectories of Infants With Multiplex Family Risk for Autism: A Baby Siblings Research Consortium Study. JAMA Neurol. 2019.
9. D’Abate L, Walker S, Yuen RKC, et al. Predictive impact of rare genomic copy number variations in siblings of individuals with autism spectrum disorders. Nat Commun. 2019;10(1):5519.
10. Gabard-Durnam LJ, Wilkinson C, Kapur K, Tager-Flusberg H, Levin AR, Nelson CA. Longitudinal EEG power in the first postnatal year differentiates autism outcomes. Nat Commun. 2019;10(1):4188.
11. McKinnon CJ, Eggebrecht AT, Todorov A, et al. Restricted and Repetitive Behavior and Brain Functional Connectivity in Infants at Risk for Developing Autism Spectrum Disorder. Biol Psychiatry Cogn Neurosci Neuroimaging. 2019;4(1):50-61.
12. Hyman SL, Levy SE, Myers SM. Identification, Evaluation, and Management of Children With Autism Spectrum Disorder. Pediatrics. 2019:e20193447.
13. Achenie LEK, Scarpa A, Factor RS, Wang T, Robins DL, McCrickard DS. A Machine Learning Strategy for Autism Screening in Toddlers. J Dev Behav Pediatr. 2019;40(5):369-376.
14. Rea KE, Armstrong-Brine M, Ramirez L, Stancin T. Ethnic Disparities in Autism Spectrum Disorder Screening and Referral: Implications for Pediatric Practice. J Dev Behav Pediatr. 2019;40(7):493-500.
15. Egger HL, Dawson G, Hashemi J, et al. Automatic emotion and attention analysis of young children at home: a ResearchKit autism feasibility study. NPJ Digit Med. 2018;1:20.
16. Dawson G, Sapiro G. Potential for Digital Behavioral Measurement Tools to Transform the Detection and Diagnosis of Autism Spectrum Disorder. JAMA Pediatr. 2019;173(4):305-306.
17. Sabatos-DeVito M, Murias M, Dawson G, et al. Methodological considerations in the use of Noldus EthoVision XT video tracking of children with autism in multi-site studies. Biol Psychol. 2019;146:107712.
18. Young GS, Constantino JN, Dvorak S, et al. A video-based measure to identify autism risk in infancy. J Child Psychol Psychiatry. 2019.
19. Guthrie W, Wallis K, Bennett A, et al. Accuracy of Autism Screening in a Large Pediatric Network. Pediatrics. 2019;144(4).
20. Lai MC, Kassee C, Besney R, et al. Prevalence of co-occurring mental health diagnoses in the autism population: a systematic review and meta-analysis. Lancet Psychiatry. 2019;6(10):819-829.
21. Kushki A, Anagnostou E, Hammill C, et al. Examining overlap and homogeneity in ASD, ADHD, and OCD: a data-driven, diagnosis-agnostic approach. Transl Psychiatry. 2019;9(1):318.
22. Koshiyama D, Fukunaga M, Okada N, et al. White matter microstructural alterations across four major psychiatric disorders: mega-analysis study in 2937 individuals. Mol Psychiatry. 2019.
23. Vasa RA, Hagopian L, Kalb LG. Investigating Mental Health Crisis in Youth with Autism Spectrum Disorder. Autism Res. 2019.
24. Maddox BB, Crabbe S, Beidas RS, et al. “I wouldn’t know where to start”: Perspectives from clinicians, agency leaders, and autistic adults on improving community mental health services for autistic adults. Autism. 2019:1362361319882227.
25. Brookman-Frazee L, Roesch S, Chlebowski C, Baker-Ericzen M, Ganger W. Effectiveness of Training Therapists to Deliver An Individualized Mental Health Intervention for Children With ASD in Publicly Funded Mental Health Services: A Cluster Randomized Clinical Trial. JAMA Psychiatry. 2019;76(6):574-583.
26. Nahmias AS, Pellecchia M, Stahmer AC, Mandell DS. Effectiveness of community-based early intervention for children with autism spectrum disorder: a meta-analysis. J Child Psychol Psychiatry. 2019;60(11):1200-1209.
27. Forsyth JK, Nachun D, Gandal MJ, et al. Synaptic and Gene Regulatory Mechanisms in Schizophrenia, Autism, and 22q11.2 Copy Number Variant-Mediated Risk for Neuropsychiatric Disorders. Biol Psychiatry. 2019.
28. Schork AJ, Won H, Appadurai V, et al. A genome-wide association study of shared risk across psychiatric disorders implicates gene regulation during fetal neurodevelopment. Nat Neurosci. 2019;22(3):353-361.
29. Walker RL, Ramaswami G, Hartl C, et al. Genetic Control of Expression and Splicing in Developing Human Brain Informs Disease Mechanisms. Cell. 2019;179(3):750-771 e722.
30. Grove J, Ripke S, Als TD, et al. Identification of common genetic risk variants for autism spectrum disorder. Nat Genet. 2019;51(3):431-444.
31. Douzgou S, Liang HW, Metcalfe K, et al. The clinical presentation caused by truncating CHD8 variants. Clin Genet. 2019;96(1):72-84.
32. Clifford H, Dulneva A, Ponting CP, Haerty W, Becker EBE. A gene expression signature in developing Purkinje cells predicts autism and intellectual disability comorbidity status. Sci Rep. 2019;9(1):485.
33. Arnett AB, Rhoads CL, Hoekzema K, et al. The autism spectrum phenotype in ADNP syndrome. Autism Res. 2018;11(9):1300-1310.
34. Feliciano P, Zhou X, Astrovskaya I, et al. Exome sequencing of 457 autism families recruited online provides evidence for autism risk genes. NPJ Genom Med. 2019;4:19.
35. Sanders SJ, Sahin M, Hostyk J, et al. A framework for the investigation of rare genetic disorders in neuropsychiatry. Nat Med. 2019;25(10):1477-1487.
36. Wong CCY, Smith RG, Hannon E, et al. Genome-wide DNA methylation profiling identifies convergent molecular signatures associated with idiopathic and syndromic autism in post-mortem human brain tissue. Hum Mol Genet. 2019;28(13):2201-2211.
37. Guan J, Cai JJ, Ji G, Sham PC. Commonality in dysregulated expression of gene sets in cortical brains of individuals with autism, schizophrenia, and bipolar disorder. Transl Psychiatry. 2019;9(1):152.
38. DiStasio MM, Nagakura I, Nadler MJ, Anderson MP. T lymphocytes and cytotoxic astrocyte blebs correlate across autism brains. Ann Neurol. 2019;86(6):885-898.
39. McGuinn LA, Windham GC, Kalkbrenner AE, et al. Early Life Exposure to Air Pollution and Autism Spectrum Disorder: Findings from a Multisite Case-Control Study. Epidemiology. 2019.
40. Jo H, Eckel SP, Chen JC, et al. Gestational diabetes mellitus, prenatal air pollution exposure, and autism spectrum disorder. Environ Int. 2019;133(Pt A):105110.
41. Jo H, Eckel SP, Wang X, et al. Sex-specific associations of autism spectrum disorder with residential air pollution exposure in a large Southern California pregnancy cohort. Environ Pollut. 2019;254(Pt A):113010.
42. Sessa A, Fagnocchi L, Mastrototaro G, et al. SETD5 Regulates Chromatin Methylation State and Preserves Global Transcriptional Fidelity during Brain Development and Neuronal Wiring. Neuron. 2019;104(2):271-289 e213.
43. Siu MT, Butcher DT, Turinsky AL, et al. Functional DNA methylation signatures for autism spectrum disorder genomic risk loci: 16p11.2 deletions and CHD8 variants. Clin Epigenetics. 2019;11(1):103.
44. Vogel Ciernia A, Laufer BI, Hwang H, et al. Epigenomic Convergence of Neural-Immune Risk Factors in Neurodevelopmental Disorder Cortex. Cereb Cortex. 2019.
45. Saffari A, Arno M, Nasser E, et al. RNA sequencing of identical twins discordant for autism reveals blood-based signatures implicating immune and transcriptional dysregulation. Mol Autism. 2019;10:38.
46. Tremblay MW, Jiang YH. DNA Methylation and Susceptibility to Autism Spectrum Disorder. Annu Rev Med. 2019;70:151-166.
47. Doan RN, Lim ET, De Rubeis S, et al. Recessive gene disruptions in autism spectrum disorder. Nat Genet. 2019;51(7):1092-1098.
48. Mahendiran T, Brian J, Dupuis A, et al. Meta-Analysis of Sex Differences in Social and Communication Function in Children With Autism Spectrum Disorder and Attention-Deficit/Hyperactivity Disorder. Front Psychiatry. 2019;10:804.
49. Bitsika V, Sharpley CF. Effects of Diagnostic Severity upon Sex Differences in Behavioural Profiles of Young Males and Females with Autism Spectrum Disorder. J Autism Dev Disord. 2019;49(11):4429-4440.
50. Margari L, Palumbi R, Peschechera A, et al. Sex-Gender Comparisons in Comorbidities of Children and Adolescents With High-Functioning Autism Spectrum Disorder. Front Psychiatry. 2019;10:159.
51. Geelhand P, Bernard P, Klein O, van Tiel B, Kissine M. The role of gender in the perception of autism symptom severity and future behavioral development. Mol Autism. 2019;10:16.
52. Lundstrom S, Marland C, Kuja-Halkola R, et al. Assessing autism in females: The importance of a sex-specific comparison. Psychiatry Res. 2019:112566.
53. Ottosen C, Larsen JT, Faraone SV, et al. Sex Differences in Comorbidity Patterns of Attention-Deficit/Hyperactivity Disorder. J Am Acad Child Adolesc Psychiatry. 2019;58(4):412-422 e413.
54. Smith REW, Avery JA, Wallace GL, Kenworthy L, Gotts SJ, Martin A. Sex Differences in Resting-State Functional Connectivity of the Cerebellum in Autism Spectrum Disorder. Front Hum Neurosci. 2019;13:104.
55. Lei J, Lecarie E, Jurayj J, et al. Altered Neural Connectivity in Females, But Not Males with Autism: Preliminary Evidence for the Female Protective Effect from a Quality-Controlled Diffusion Tensor Imaging Study. Autism Res. 2019;12(10):1472-1483.
56. Andrews DS, Lee JK, Solomon M, Rogers SJ, Amaral DG, Nordahl CW. A diffusion-weighted imaging tract-based spatial statistics study of autism spectrum disorder in preschool-aged children. J Neurodev Disord. 2019;11(1):32.
57. Cauvet E, Van’t Westeinde A, Toro R, et al. Sex Differences Along the Autism Continuum: A Twin Study of Brain Structure. Cereb Cortex. 2019;29(3):1342-1350.
58. Carlezon WA, Jr., Kim W, Missig G, et al. Maternal and early postnatal immune activation produce sex-specific effects on autism-like behaviors and neuroimmune function in mice. Sci Rep. 2019;9(1):16928.
59. Maddox BB, Rump KM, Stahmer AC, et al. Concordance between a U.S. Educational Autism Classification and the Autism Diagnostic Observation Schedule. J Clin Child Adolesc Psychol. 2019:1-7.
60. Kraemer BR, Odom SL, Tomaszewski B, et al. Quality of high school programs for students with autism spectrum disorder. Autism. 2019:1362361319887280.
61. Rosen TE, Spaulding CJ, Gates JA, Lerner MD. Autism severity, co-occurring psychopathology, and intellectual functioning predict supportive school services for youth with autism spectrum disorder. Autism. 2019;23(7):1805-1816.
62. Nuske HJ, Pellecchia M, Lushin V, et al. Do Student Characteristics Affect Teachers’ Decisions to Use 1:1 Instruction? J Autism Dev Disord. 2019;49(7):2864-2872.
63. Locke J, Lawson GM, Beidas RS, et al. Individual and organizational factors that affect implementation of evidence-based practices for children with autism in public schools: a cross-sectional observational study. Implement Sci. 2019;14(1):29.
64. Pellecchia M, Marcus SC, Spaulding C, et al. Randomized Trial of a Computer-Assisted Intervention for Children With Autism in Schools. J Am Acad Child Adolesc Psychiatry. 2019.
65. Locke J, Kang-Yi C, Pellecchia M, Mandell DS. It’s Messy but Real: A Pilot Study of the Implementation a Social Engagement Intervention for Children with Autism in Schools. J Res Spec Educ Needs. 2019;19(2):135-144.
66. Bilaver LA, Havlicek J. Racial and Ethnic Disparities in Autism-Related Health and Educational Services. J Dev Behav Pediatr. 2019;40(7):501-510.
67. LaClair M, Mandell DS, Dick AW, Iskandarani K, Stein BD, Leslie DL. The effect of Medicaid waivers on ameliorating racial/ethnic disparities among children with autism. Health Serv Res. 2019;54(4):912-919.
68. Black MH, Mahdi S, Milbourn B, et al. Perspectives of key stakeholders on employment of autistic adults across the united states, australia, and sweden. Autism Res. 2019;12(11):1648-1662.
69. Zaslavsky K, Zhang WB, McCready FP, et al. SHANK2 mutations associated with autism spectrum disorder cause hyperconnectivity of human neurons. Nat Neurosci. 2019;22(4):556-564.
70. Ross PJ, Zhang WB, Mok RSF, et al. Synaptic Dysfunction in Human Neurons With Autism-Associated Deletions in PTCHD1-AS. Biol Psychiatry. 2019.
71. Deneault E, White SH, Rodrigues DC, et al. Complete Disruption of Autism-Susceptibility Genes by Gene Editing Predominantly Reduces Functional Connectivity of Isogenic Human Neurons. Stem Cell Reports. 2018;11(5):1211-1225.
72. Gordon A, Forsingdal A, Klewe IV, et al. Transcriptomic networks implicate neuronal energetic abnormalities in three mouse models harboring autism and schizophrenia-associated mutations. Mol Psychiatry. 2019.
73. Kim JW, Park K, Kang RJ, et al. Gene-environment interaction counterbalances social impairment in mouse models of autism. Sci Rep. 2019;9(1):11490.
74. Mohammadi S, Asadi-Shekaari M, Basiri M, Parvan M, Shabani M, Nozari M. Improvement of autistic-like behaviors in adult rats prenatally exposed to valproic acid through early suppression of NMDA receptor function. Psychopharmacology (Berl). 2019.
75. Tang S, Terzic B, Wang IJ, et al. Altered NMDAR signaling underlies autistic-like features in mouse models of CDKL5 deficiency disorder. Nat Commun. 2019;10(1):2655.
76. Xing X, Zhang J, Wu K, et al. Suppression of Akt-mTOR pathway rescued the social behavior in Cntnap2-deficient mice. Sci Rep. 2019;9(1):3041.
77. Talbott MR, Dufek S, Zwaigenbaum L, et al. Brief Report: Preliminary Feasibility of the TEDI: A Novel Parent-Administered Telehealth Assessment for Autism Spectrum Disorder Symptoms in the First Year of Life. J Autism Dev Disord. 2019.
78. Mazurek MO, Stobbe G, Loftin R, et al. ECHO Autism Transition: Enhancing healthcare for adolescents and young adults with autism spectrum disorder. Autism. 2019:1362361319879616.
79. Reddihough DS, Marraffa C, Mouti A, et al. Effect of Fluoxetine on Obsessive-Compulsive Behaviors in Children and Adolescents With Autism Spectrum Disorders: A Randomized Clinical Trial. JAMA. 2019;322(16):1561-1569.
80. Herscu P, Handen BL, Arnold LE, et al. The SOFIA Study: Negative Multi-center Study of Low Dose Fluoxetine on Repetitive Behaviors in Children and Adolescents with Autistic Disorder. J Autism Dev Disord. 2019.
81. Bolognani F, Del Valle Rubido M, Squassante L, et al. A phase 2 clinical trial of a vasopressin V1a receptor antagonist shows improved adaptive behaviors in men with autism spectrum disorder. Sci Transl Med. 2019;11(491).
82. Carpenter KLH, Major S, Tallman C, et al. White Matter Tract Changes Associated with Clinical Improvement in an Open-Label Trial Assessing Autologous Umbilical Cord Blood for Treatment of Young Children with Autism. Stem Cells Transl Med. 2019;8(2):138-147.
83. Kang DW, Adams JB, Coleman DM, et al. Long-term benefit of Microbiota Transfer Therapy on autism symptoms and gut microbiota. Sci Rep. 2019;9(1):5821.
84. Sharon G, Cruz NJ, Kang DW, et al. Human Gut Microbiota from Autism Spectrum Disorder Promote Behavioral Symptoms in Mice. Cell. 2019;177(6):1600-1618 e1617.
85. Arnold LE, Luna RA, Williams K, et al. Probiotics for Gastrointestinal Symptoms and Quality of Life in Autism: A Placebo-Controlled Pilot Trial. J Child Adolesc Psychopharmacol. 2019;29(9):659-669.
86. Pretzsch CM, Voinescu B, Mendez MA, et al. The effect of cannabidiol (CBD) on low-frequency activity and functional connectivity in the brain of adults with and without autism spectrum disorder (ASD). J Psychopharmacol. 2019;33(9):1141-1148.