Autism diagnosis at 3 years of age isn’t something that happens suddenly. It evolves, there are deficits seen early on and markers that are evident prior to 3 years. Some of them are cascading events – with problems in one area like motor function, other behaviors like reaching, grasping, and learning about the environment and interactions with other people are stunted. Sometimes, these cascading moments lead to a loss of language. Early intervention can turn these early deficits around so that communication, learning and daily functioning are continually supported and instead of one trajectory, another can be reached. This podcast highlights studies that demonstrate that with data, and with theory. But it is never boiled down to one thing, despite early studies that screen time use is linked with an ASD diagnosis. Listen to the podcast here.
This week is a “brick-a-brack”: of topics. They include: 1. how COVID-19 is especially dangerous for people with neurodevelopmental disorders; 2. how certain genes associated with neurodevelopmental disorders can affect other body functions other than the brain (like the digestive system and kidney function and metabolism); and finally, 3. why parents think their autistic children are so great. No overall theme, just information we hope you can use. Listen to the podcast here.
Parents are now used as intervention partners through a design called parent-mediated intervention. It started to be studied before the pandemic but has now become a necessity. Does it work? Should it always work for everything? How long should the intervention last and how often? These are all questions of interest, and while research is still early, parents can be amazing partners in intervention especially below age 5. The provide opportunities for learning and communication, and they can utilize more hours during the day at home than traditional in-clinic services can. Of course not every family is the same and may not have the same abilities to learn the intervention, and in the future more of these contextual factors need to be studied. But for now, three cheers for parents helping their kids! Listen to the podcast here.
This week, we talk to Karla Rivera-Figueroa and Inge-Marie Eigsti, who together with Nana Yaa A. Marfo published a systematic review asking about parental perceptions of autism in both LatinX and Black Sociocultural contexts. Six themes popped out, and the question for Karla and Dr Eigsti were “how can research help”? What funding opportunities, culturally relevant materials, and future research directions need to be focused on? The conversation included ways to battle stigma, improve provider relationships, recruit a more diverse sample in research and fund those underrepresented scientists who want to study autism. As a note, ASF will be releasing their undergraduate fellowship mechanism on Tuesday which will focus on underrepresented groups. Listen to the podcast here.
Most people with autism have some sort of sensory dysfunction: hypersensitivity or hyposensitivity or sensory avoiding behaviors to touch, smell, sound, light. But a new study looking at kids from the Study to Explore Early Development (SEED) suggest that it may be more important than you think. In fact, it was the only feature to unify those with autism compared to those with developmental delay. Are there treatments outside of environmental supports to help sensory issues? There could be: a drug that tried and failed to treat other features of autism called arbacolfen supports the idea that this drug target could be helpful in treating sensory issues. Listen to the podcast here.
A Summary of Autism Discoveries in 2016 and What It Means for Families
By Alycia Halladay, PhD, Chief Science Officer of the Autism Science Foundation and the Scientific Advisory Board of the Autism Science Foundation
To listen to our year-end research summary podcast, click here.
For decades, the autism community has known that autism affects the entire family. Biological parents have been included in autism studies to examine where genetic mutations come from, but always with an eye for understanding the affected individual. This year in research saw a much bigger focus on family members of those with autism, particularly siblings. The goal of these studies is to understand the genetic and biological nature of autism so that help can be provided not just to those with a diagnosis, but to family members as well.
Many studies focused on what is known as the “broader autism phenotype,” previously explored in biological parents. The “broader autism phenotype” refers to some behavioral features of autism, including those in emotion, language, and social skills that do not meet the level of a diagnosis of autism spectrum disorder. Rather, they have been termed anything from “intermediate” autism to “a hint of autism.” Joe Piven and James Harris hypothesized this year that Bruno Bettleheim may have tragically misinterpreted these features, in the absence of a true understanding of autism, as “refrigerator mothers.” Clinicians have urged scientists to note these symptoms in a way that does not create a new diagnostic category and noting certain social, personality and language characteristics in family members has been crucial for nailing down the underlying biology.
Importantly, significant scientific discoveries in autism were made possible by looking directly at the brains of people with autism. This type of research has been made possible through the Autism BrainNet. This summary highlights the important role of studying brain tissue from individuals with autism to better understand people with autism across the lifespan, including those with known causes and unknown causes of autism spectrum disorder (ASD). See the section below entitled “Using brain tissue to understand causes of ASD” for more details on findings from brain tissue research in 2016.
Siblings show features of autism, but not to worry
This year, four studies assessed the broader autism phenotype in siblings, and other studies went further to look at psychiatric symptoms in siblings who were not diagnosed with autism. In the past, researchers mistakenly believed that siblings showed no symptoms of autism. In fact, adolescent, school age, and adult siblings of those with autism show elevated autism symptoms [1, 2] as well as categorical features of autism similar to those seen with autism [3], compared to those with no family history. High-risk infant sibling studies have shown that siblings of toddlers with autism, while not diagnosed with autism, have a higher rate of autism spectrum disorder (ASD) symptoms [4].
This is also consistent with the broader autism phenotype, with the last study indicating that sibling symptoms are observed across the lifespan. Unfortunately, signs of the broader autism phenotype puts siblings at risk for internalizing and externalizing behaviors like depression, psychological problems, and other behavioral issues [5, 6]. In addition to anxiety and depression, research this year showed increased risk of psychiatric comorbidities including ADHD and substance abuse disorders [7-9]. On the other hand, siblings who were within the typical range of Social Responsiveness Scale (SRS) scores didn’t show elevated sensory issues [10]. The goal of studying siblings of those with autism, again, is not to look for features which pathologize them, but to help identify features, challenges, and strengths that help them. Research published previously identifies the unique nature of sibling relationships, in that siblings of a person with autism view their relationship positively across the lifespan, whereas siblings of typically developing individuals tend to report positive feelings at a decreased rate in adulthood [11].
Understanding the causes of autism by studying sex differences
In addition to understanding siblings to help develop specialized services and supports, learning about siblings can help researchers understand the causes of autism and, specifically, why females are less likely to be diagnosed compared to males. New prevalence data from the CDC showed that the prevalence of autism is again at 1:68, perhaps showing a plateau in the rates of autism in the US. However, the difference in the rates between males and females still hovers around 4:1 depending on IQ [12]. Researchers this year showed that females may be able to hide symptoms because of better social abilities [13] and because they may be protected in some way from certain symptoms [14]. For example, those studying infants at risk for autism show that baby girls with autism show increased attention to social stimuli compared to baby boys [15]. This difference may affect how they express symptoms later on. Finally, preliminary studies this year suggest a slight bias in diagnostic instruments [16] and evidence of camouflaging autism symptoms in females [17].
There are likely multiple reasons behind the male sex bias in autism, but few have received any empirical study. This year, the Autism Sisters Project began recruiting at the Icahn School of Medicine at Mount Sinai. This study is poised to understand why females are not diagnosed as often, including differences in IQ and underlying genetic factors. Of importance, the study is focusing on the undiagnosed sister of individuals with ASD. As much as studying siblings with autism may help researchers understand sex differences in autism, so will actually studying males and females with ASD. Donna Werling from USCF looked at genes expressed in the brains of males and females with and without autism to understand sex differences in gene expression, particularly in those genes associated with autism. She found that it was not ASD risk genes that show differences, but those that are involved in neural pathways associated with autism, like microglia and the immune system, that show sex differences. The male bias in this gene expression may be what modulates ASD risk [18]. A male sex bias is not unusual across neurodevelopmental disorders, and so understanding its role in autism diagnoses may be informative of disorders like ADHD and anxiety as well. Just like there are fewer females diagnosed with autism, there are fewer brains of females to study, slowing scientists’ understanding of ASD. In order to learn more about how women with ASD can participate, click here.
More to learn about genetics associated with ASD
Even more new risk genes were discovered this year, and/or replicated in different cohorts. These investigations went beyond “autism” vs. “no autism” to specific features of autism, with the goal of understanding what genes lead to what behavioral features of ASD. For example, several studies found associations between a gene called POGZ and autism, particularly autism with intellectual disability [19-23]. POGZ is a gene that makes a protein that affects the expression of other genes. Therefore, the mutation of this gene produces disruption in the expression of several genes, rather than just one. Similar specific behavioral features are found with mutations of TRIP12 or DYRK1A, which also leads to widespread, rather than specific, changes in gene expression with a particular form of autism: autism with intellectual disability [24, 25]. By further investigating individuals for whom substantial amounts of data is available, including cognitive ability and comorbid medical conditions, the causes of these features will be better understood and will hopefully lead to better treatments. Researchers have also better identified how genes seen in other disorders but cause autism are transmitted, for example via maternal [26, 27] or paternal [28] pathways, influenced by things like paternal age [29], which might aid genetic counseling. Contrary to this idea, however, is the finding that individuals with either a known genetic cause of autism or autism where there is no known cause (i.e., idiopathic) have a considerable amount of overlap in mutations in the brain which affect how genes are turned on and off – in other words “epimutations” [29, 30]. This is further evidence that beyond the way DNA is sequenced, factors that affect how genes are activated are important to autism etiology as well. Epigenetic markers are known to be sensitive to environmental exposures of different types and insight into these pathways continue to open the door to understanding gene/environment interactions in autism.
And it’s not just about pure genetics, it’s about interactions between genes and the environment.
Genetics plays a huge role in the causes of autism, but this year researchers dove even deeper into the multifactorial causes of autism, specifically the role of genetics and the environment. The environment includes, broadly speaking, anything from toxic chemicals to age of the parent. It includes sociological, pharmacological, toxicological, and medical exposures.
This year saw two epidemiological studies examining the interaction between genes and the environment, but this time the investigation expanded to include who carried the genetic mutation and how autism was defined. First, studying the genotype of mothers showed that a particular mutation of the serotonin receptor gene and a high level of stressors during pregnancy produced a higher risk for having a child with autism than those without this same mutation [31]. Rather than using these factors to understand autism risk, others are going beyond to understand symptoms within autism. For example, using the Simons Simplex Collection, scientists showed that boys with autism who had genetic markers of mutations called copy number variations, together with exposure to an environmental exposure, showed the most severe autism symptoms, marked by repetitive behaviors and cognitive challenges [32]. The study is the first to look at type and severity of symptoms following multiple risk factors rather than a diagnosis, and the idea of understanding multiple risk factors for symptoms, rather than diagnosis itself, needs further study. Animal models of autism found that paternal age, a commonly accepted risk factor for autism spectrum disorder, combined with a mutation of a gene that affects synaptic development, results in certain symptoms of ASD in this model [33]. More fine-grained analysis of autism symptoms, rather than an autism diagnosis per-se, is needed to better understand the causes of autism. It’s also important to understand environmental factors because in some cases, like those of chemical and toxicological exposures, these can be controlled through regulatory means. Many studies have linked air pollution to autism [34] and in early July a landmark consensus statement authored by over 30 scientists, physicians, and public health experts was published which calls for the reduction of toxic chemical exposures to possibly reduce the risk of many developmental disorders [35]. So far, the only established way to protect against autism has been dietary folic acid supplementation [36], so reduction of modifiable risk factors should be a focus of future public health research.
Another potentially modifiable risk factor is maternal infection during pregnancy. Of course, not all cases of maternal infection are preventable, but some of them are. This year, a study revealed that neither having the flu, nor being vaccinated against the flu during pregnancy, was shown to contribute to autism risk in children [37]. However, maternal immune response during pregnancy was linked to a specific behavioral phenotype of autism, specifically those with intellectual disabilities [38]. According to animal models, the effects of altering the immune system function early in cell formation may lead to longer lasting elevations in chemokines (which are immune chemicals associated with autism) than previously thought [39]. This may be attributed to long lasting changes in gene expression patterns, regulated via epigenetic mechanisms [40, 41], resulting in an increase of methylation of genes and producing effects across generations. These findings converge with other research that demonstrates similar methylation patterns in individuals with ASD, even without immune system challenges during early life.
For years, some autism researchers have observed the presence of antibodies to brain tissue in some mothers of children with autism. This year, researchers looking at animal models discovered that they may be acting through an autism risk gene [42]. Also, the increased risk may be particularly elevated in mothers with specific medical conditions [43]. While scientists remain cautious about translating these findings to a commercialized method of determining autism risk, they continue to provide insights into the neurobiology of autism, and especially the immune system.
Using brain tissue to understand causes of ASD
Brain tissue research will also help researchers better identify causes of different types of autism so that better treatments can be developed. For example, one of the more challenging and debilitating medical comorbidities associated with autism is seizures and epilepsy. A study of brains of individuals with both autism and autism and epilepsy show increased numbers of glial cells. These cells are not neurons, rather they provide support and protection to brain cells [44]. The glial cell numbers were highest in those with restricted and repetitive behaviors, but, interestingly enough, the number of glia go down over time in individuals with autism, but up in those without autism. This suggests that the glial cells contribute to autism severity and cause. Similar comparisons to other disorders associated with autism were made studying amyloid B precursor protein and their metabolites. These molecules are associated with Alzheimer’s disease but also have a host of other functions that are not pathogenic. For example, they can affect neuroinflammation and normal cellular activity. In autism, levels of these proteins were reduced in brain and plasma, but elevated in individuals with Fragile X syndrome [45]. This suggests that these amyloid B proteins are involved with both disorders, and may be a target of interventions in the future.
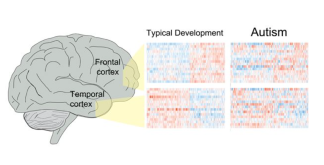
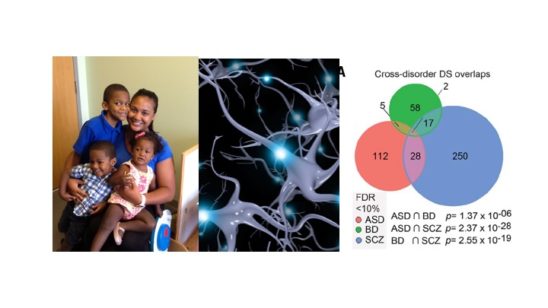
Figure found in Parikshak et al., 2016
Brain tissue research goes beyond identifying treatment targets to helping researchers understand how the brains of people with autism work on a cellular level. This year, two studies demonstrated that in addition to mutations in autism risk genes, mutations in areas of the gene that control the function of autism risk genes are also affected [30, 46]. What is also interesting is that regardless of the symptoms or causes of autism, the pattern of gene activity was similar in those with autism, validating a much smaller study from years ago [46]. These results also reiterate the importance of early intervention for treatment of debilitating autism symptoms, since both genes identified recently that control brain development peak during the first few years of life. It is important for all families, regardless of whether or not they are directly affected by autism, to learn more about brain tissue donation. You can register for more information by clicking here.
Should clinicians think in terms of autism diagnosis, or in terms of symptoms?
This year showed the shared features between autism and many other disorders like Phelan-McDermid syndrome, mutations of chromosome 16, Dup15, and even schizophrenia. In particular, disorders don’t just share autism symptoms; they show similar neurological and cognitive features as well [27, 47]. So how much is specific to autism, and how much is related to behavioral, neurological, and other medical issues that are seen without an autism diagnosis? And do these genetic findings explain certain symptoms associated with autism, but not core to autism? It has been argued that classifying individuals based on specific symptom dimensions, such as the presence of abnormal behaviors, absence of other behaviors, and cognitive ability may help clinicians better distinguish cross disorders [48, 49]. This idea is not new, with a recent movement towards a new way of thinking towards autism diagnosis [50]. New findings from the brains of individuals with a diagnosis of autism or schizophrenia show significant overlap between the gene transcription in the brains of people with either autism or schizophrenia, but not bipolar disorder [51]. The authors conclude that these two disorders share many genes associated with synapse development, and the formation of connections across different brain regions. Therefore, these disorders may not be totally different at the biological level. Rather than thinking of autism as a whole, early signs of autism can also be linked to specific genetic markers, which may explain autism symptoms, but not autism as a diagnosis. This includes mutations of the oxytocin receptor on later empathy [52] and dopamine receptors on a core feature – initiating joint attention [53]. This idea has enormous implications for autism research and treatment, as it implies a switch in the way autism is identified. It has been suggested that behavioral symptoms, combined with biological and environmental variables, should be combined to lead to categories, rather than diagnosis of disorders. This is called Research Domain Criteria, or RDOC.
Autism can also be very difficult to diagnose, but this year two new studies suggested that the process can be streamlined, at least a little bit. In school age verbal children, a new instrument called the Autism Symptom Inventory (ASI) was good at diagnosing autism in about 20 minutes [54]. Another instrument, which doesn’t have a name yet, combines three short instruments (including the ASI) and was also promising, especially in terms of studies aiming to understand the causes of autism, both genetic and environmental [55]. These studies offer hope to large scale epidemiological studies seeking to identify and characterize individuals with autism, although right now their ability to identify different subtypes which may be amenable to specialized treatments is limited.
When it comes to intervention, earlier is best, but not the only option
The most remarkable evidence of the effectiveness of early intervention has come from longitudinal studies – those that study an intervention YEARS after it was delivered. If early intervention improves brain connectivity and allows for connections to be formed to alleviate autism symptoms, the effects may not be seen right away – it may take years. They can take the form of an intervention study that follows families for a long time, or by investigating factors early on that predicted improvement at school age and beyond. This year saw both. In 2010, a gold standard randomized clinical trial study out of the UK looked at a parent-delivered intervention focusing on communication, and, while they found it showed promise, it didn’t produce improvements in symptom severity [56]. The initial findings were hopeful, but also disappointing. However, when they followed up on these children five years later, the training of the parents to deliver the intervention resulted in a reduction of autism symptoms [57]. The findings are important for many reasons. First, autism intervention is a journey, not necessarily a destination, and interventions delivered early on may alter the trajectory of symptoms [57]. Second, parents can deliver interventions in a wide variety of settings in a way that is more intensive than limited clinic time, and an intervention targeted at one set of autism symptoms like social communication may also affect others like repetitive behaviors [58]. This does not mean that trained Applied Behavioral Analysis (ABA) therapists and intervention delivered by trained professionals should be abandoned. Parent-delivered interventions are a supplement at ages when kids spend most of their time with parents rather than schools. Another important thing to remember about early intervention is that more data published this year shows that for a percentage of children, a diagnosis is not possible at two years of age. A group of children who show some symptoms but don’t meet criteria at two years of age do end up with a diagnosis by three years of age [59] despite being seen by well-trained, very experienced clinicians. Early intervention may help those who don’t have an actual autism diagnosis yet. Studying infants with autism has also been instrumental in determining not only interventions, but the nature of autism itself. For years, people assumed that the reduced eye contact in people with autism was because they were actively averting the eyes, found eye contact aversive, and didn’t want to look at the gaze of the other person. However, this isn’t the case. At least early in life, infants with autism don’t actively avert gaze, they just aren’t that interested in looking at the eyes and don’t get the same social signals from eye contact as those with autism do [60].
Parents as methods of treatment delivery
Parent-delivered interventions can be used at different times, again to supplement, rather than replace, other treatments delivered in clinical settings. Parent training, not the less intensive parent education, on behavior management techniques improved adaptive behavior and daily living in children with autism. However, these gains were mostly seen in those with average intellectual functioning [61]. This suggests that not all individuals respond to parent-delivered interventions. And it isn’t just used in isolation. It enhances the efficacy of drugs to alleviate ADHD in those with autism [62]. Parent training may seem like an easy solution, but in the real world setting of parents and trainers, it is very complicated [63].
What can predict who will respond to what treatment?
There have also been advances in pharmacological treatments of autism, but they always struggle with improving behavior or outcome, not specific to core autism symptoms. Oxytocin, a naturally occurring hormone, has shown mixed results in improving different aspects of autism-related behavior, including face recognition, social behavior, and empathy [64]. Looking at the effect of oxytocin on the brain, it improves connectivity between areas of the brain involved in reward and those involved in perception of social communication cues in children with autism [65]. However, it isn’t simple, and, as it turns out, that makes the story more promising. People with mutations of the oxytocin receptor have different types of mutations. These different types of mutations in people with autism lead to different patterns of this connectivity [66] as well as the ability to recognize faces [67]. Finally, these different mutations also predict the behavioral response to oxytocin – in other words, whether or not this hormone produces improvements in social abilities [68]. These different studies are a perfect illustration of how personalized medicine will improve autism treatment. Those with particular types of genetic differences will respond better to oxytocin treatment than others, which will speed up people receiving the right type of intervention.
In addition to genetic markers predicting treatment response, advances in other biomarkers to predict treatment response have been made as well. Individuals who were more responsive to Pivotal Response Treatment (PRT) showed a specific pattern of pre-treatment brain activity when presented with a social situation on a video [69]. In fact, it predicted response to treatment better than any baseline behavioral measures. In the future, just like looking at the genetic makeup of people with autism, understanding their underlying brain function before treatment can help get the people into the treatments that would benefit them the most.
The whole purpose of improvements in autism diagnosis and interventions is to deliver services to individuals that need them. So, how are insurance mandates doing in terms of identifying individuals with autism and providing them with the treatments they need? This year, David Mandell at the University of Pennsylvania demonstrated with data obtained through insurance companies that these mandates are increasing the number of people receiving services. That’s the good news. The bad news is that the increase is not nearly as much as it should be keeping in pace with the prevalence of autism. So, he concludes, these mandates are necessary but not sufficient to provide services to all that need them [70]. In addition, there are acknowledged gaps in what pediatricians know about non-medical treatments and services in their areas, and what parents need them to understand [71].
In summary, this year saw research that helps understand the causes of autism; includes siblings to provide better services to the entire family; showed promise of the concept of “personalized medicine” everyone has heard so much about; demonstrated the long term, not just short term effects of behavioral interventions and the importance of parents and caregivers; and emphasized the need to better understand features of individuals with autism rather than just the straight diagnosis of ASD.
References:
Ruzich, E., et al., The Autism-Spectrum Quotient in siblings of people with Autism. Autism Res, 2016. 9(10): p. 1114.
Ruzich, E., et al., Subgrouping siblings of people with autism: Identifying the broader autism phenotype. Autism Res, 2016. 9(6): p. 658-65.
Tsang, T., K. Gillespie-Lynch, and T. Hutman, Theory of Mind Indexes the Broader Autism Phenotype in Siblings of Children with Autism at School Age. Autism Res Treat, 2016. 2016: p. 6309189.
Charman, T., et al., Non-ASD outcomes at 36 months in siblings at familial risk for autism spectrum disorder (ASD): A baby siblings research consortium (BSRC) study. Autism Res, 2016.
Walton, K.M., Risk Factors for Behavioral and Emotional Difficulties in Siblings of Children With Autism Spectrum Disorder.Am J Intellect Dev Disabil, 2016. 121(6): p. 533-549.
Fullerton, J.M., et al., Siblings of children with life-limiting conditions: psychological adjustment and sibling relationships.Child Care Health Dev, 2016.
Jokiranta-Olkoniemi, E., et al., Risk of Psychiatric and Neurodevelopmental Disorders Among Siblings of Probands With Autism Spectrum Disorders. JAMA Psychiatry, 2016. 73(6): p. 622-9.
Butwicka, A., et al., Increased Risk for Substance Use-Related Problems in Autism Spectrum Disorders: A Population-Based Cohort Study. J Autism Dev Disord, 2016.
Miller, M., et al., School-age outcomes of infants at risk for autism spectrum disorder. Autism Res, 2016. 9(6): p. 632-42.
Hilton, C.L., et al., Sensory Responsiveness in Siblings of Children with Autism Spectrum Disorders. J Autism Dev Disord, 2016.
Seltzer, M.M., G.I. Orsmond, and A.J. Esbensen, Siblings of individuals with an autism spectrum disorder: Sibling relationships and wellbeing in adolescence and adulthood. Autism : the international journal of research and practice, 2009. 13(1): p. 59-80.
Christensen, D.L., et al., Prevalence and Characteristics of Autism Spectrum Disorder Among Children Aged 8 Years–Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2012. MMWR Surveill Summ, 2016. 65(3): p. 1-23.
Rynkiewicz, A., et al., An investigation of the ‘female camouflage effect’ in autism using a computerized ADOS-2 and a test of sex/gender differences. Mol Autism, 2016. 7: p. 10.
Constantino, J.N., Data from the Baby Siblings Research Consortium confirm and specify the nature of the female protective effect in autism: A commentary on Messinger et al. Mol Autism, 2016. 7: p. 32.
Chawarska, K., et al., Enhanced Social Attention in Female Infant Siblings at Risk for Autism. J Am Acad Child Adolesc Psychiatry, 2016. 55(3): p. 188-95 e1.
Beggiato, A., et al., Gender differences in autism spectrum disorders: Divergence among specific core symptoms. Autism Res, 2016.
Lai, M.C., et al., Quantifying and exploring camouflaging in men and women with autism. Autism, 2016.
Werling, D.M., N.N. Parikshak, and D.H. Geschwind, Gene expression in human brain implicates sexually dimorphic pathways in autism spectrum disorders. Nat Commun, 2016. 7: p. 10717.
Wang, T., et al., De novo genic mutations among a Chinese autism spectrum disorder cohort. Nat Commun, 2016. 7: p. 13316.
Stessman, H.A., et al., Disruption of POGZ Is Associated with Intellectual Disability and Autism Spectrum Disorders. Am J Hum Genet, 2016. 98(3): p. 541-52.
Loviglio, M.N., et al., Identification of a RAI1-associated disease network through integration of exome sequencing, transcriptomics, and 3D genomics. Genome Med, 2016. 8(1): p. 105.
Tan, B., et al., A novel de novo POGZ mutation in a patient with intellectual disability. J Hum Genet, 2016. 61(4): p. 357-9.
Hashimoto, R., et al., Whole-exome sequencing and neurite outgrowth analysis in autism spectrum disorder. J Hum Genet, 2016. 61(3): p. 199-206.
Bramswig, N.C., et al., Identification of new TRIP12 variants and detailed clinical evaluation of individuals with non-syndromic intellectual disability with or without autism. Hum Genet, 2016.
van Bon, B.W., et al., Disruptive de novo mutations of DYRK1A lead to a syndromic form of autism and ID. Mol Psychiatry, 2016. 21(1): p. 126-32.
Connolly, S., et al., A genome-wide investigation into parent-of-origin effects in autism spectrum disorder identifies previously associated genes including SHANK3. Eur J Hum Genet, 2016.
Duyzend, M.H., et al., Maternal Modifiers and Parent-of-Origin Bias of the Autism-Associated 16p11.2 CNV. Am J Hum Genet, 2016. 98(1): p. 45-57.
Isles, A.R., et al., Parental Origin of Interstitial Duplications at 15q11.2-q13.3 in Schizophrenia and Neurodevelopmental Disorders. PLoS Genet, 2016. 12(5): p. e1005993.
Yuen, R.K., et al., Genome-wide characteristics of de novo mutations in autism. NPJ Genom Med, 2016. 1: p. 160271-1602710.
Sun, W., et al., Histone Acetylome-wide Association Study of Autism Spectrum Disorder. Cell, 2016. 167(5): p. 1385-1397 e11.
Hecht, P.M., et al., Maternal serotonin transporter genotype affects risk for ASD with exposure to prenatal stress. Autism Res, 2016. 9(11): p. 1151-1160.
Jane Webb, S., et al., Severity of ASD symptoms and their correlation with the presence of copy number variations and exposure to first trimester ultrasound. Autism Research, 2016: p. n/a-n/a.
Yoshizaki, K., et al., Paternal Aging Affects Behavior in Pax6 Mutant Mice: A Gene/Environment Interaction in Understanding Neurodevelopmental Disorders. PLoS One, 2016. 11(11): p. e0166665.
Lam, J., et al., A Systematic Review and Meta-Analysis of Multiple Airborne Pollutants and Autism Spectrum Disorder. PLoS One, 2016. 11(9): p. e0161851.
Bennett, D., et al., Project TENDR: Targeting Environmental Neuro-Developmental Risks The TENDR Consensus Statement.Environ Health Perspect, 2016. 124(7): p. A118-22.
Gao, Y., et al., New Perspective on Impact of Folic Acid Supplementation during Pregnancy on Neurodevelopment/Autism in the Offspring Children – A Systematic Review. PLoS One, 2016. 11(11): p. e0165626.
Zerbo, O., et al., Association Between Influenza Infection and Vaccination During Pregnancy and Risk of Autism Spectrum Disorder. JAMA Pediatr, 2016.
Jones, K.L., et al., Autism with intellectual disability is associated with increased levels of maternal cytokines and chemokines during gestation. Mol Psychiatry, 2016.
Rose, D.R., et al., Long-term altered immune responses following fetal priming in a non-human primate model of maternal immune activation. Brain Behav Immun, 2016.
Weber-Stadlbauer, U., et al., Transgenerational transmission and modification of pathological traits induced by prenatal immune activation. Mol Psychiatry, 2016.
Richetto, J., et al., Genome-wide DNA Methylation Changes in a Mouse Model of Infection-Mediated Neurodevelopmental Disorders. Biol Psychiatry, 2016.
Brimberg, L., et al., Caspr2-reactive antibody cloned from a mother of an ASD child mediates an ASD-like phenotype in mice.Mol Psychiatry, 2016. 21(12): p. 1663-1671.
Krakowiak, P., et al., Autism-specific maternal anti-fetal brain autoantibodies are associated with metabolic conditions. Autism Res, 2016.
Menassa, D.A., C. Sloan, and S.A. Chance, Primary olfactory cortex in autism and epilepsy: increased glial cells in autism. Brain Pathol, 2016.
Ray, B., et al., Finding novel distinctions between the sAPPalpha-mediated anabolic biochemical pathways in Autism Spectrum Disorder and Fragile X Syndrome plasma and brain tissue. Sci Rep, 2016. 6: p. 26052.
Parikshak, N.N., et al., Genome-wide changes in lncRNA, splicing, and regional gene expression patterns in autism. Nature, 2016.
Steinman, K.J., et al., 16p11.2 deletion and duplication: Characterizing neurologic phenotypes in a large clinically ascertained cohort. Am J Med Genet A, 2016. 170(11): p. 2943-2955.
Foss-Feig, J.H., et al., Re-conceptualizing ASD Within a Dimensional Framework: Positive, Negative, and Cognitive Feature Clusters. J Autism Dev Disord, 2016. 46(1): p. 342-51.
Schwarz, E., H. Tost, and A. Meyer-Lindenberg, Working memory genetics in schizophrenia and related disorders: An RDoC perspective. Am J Med Genet B Neuropsychiatr Genet, 2016. 171B(1): p. 121-31.
London, E.B., Categorical diagnosis: a fatal flaw for autism research? Trends Neurosci, 2014. 37(12): p. 683-6.
Ellis, S.E., et al., Transcriptome analysis of cortical tissue reveals shared sets of downregulated genes in autism and schizophrenia.Transl Psychiatry, 2016. 6: p. e817.
McDonald, N.M., J.K. Baker, and D.S. Messinger, Oxytocin and parent-child interaction in the development of empathy among children at risk for autism. Dev Psychol, 2016. 52(5): p. 735-45.
Gangi, D.N., et al., Dopaminergic variants in siblings at high risk for autism: Associations with initiating joint attention. Autism Res, 2016. 9(11): p. 1142-1150.
Bishop, S.L., et al., The autism symptom interview, school-age: A brief telephone interview to identify autism spectrum disorders in 5-to-12-year-old children. Autism Res, 2016.
Newschaffer, C.J., et al., Development and validation of a streamlined autism case confirmation approach for use in epidemiologic risk factor research in prospective cohorts. Autism Res, 2016.
Green, J., et al., Parent-mediated communication-focused treatment in children with autism (PACT): a randomised controlled trial. Lancet, 2010. 375(9732): p. 2152-60.
Pickles, A., et al., Parent-mediated social communication therapy for young children with autism (PACT): long-term follow-up of a randomised controlled trial. Lancet, 2016.
Harrop, C., et al., The impact of caregiver-mediated JASPER on child restricted and repetitive behaviors and caregiver responses.Autism Res, 2016.
Zwaigenbaum, L., et al., Stability of diagnostic assessment for autism spectrum disorder between 18 and 36 months in a high-risk cohort. Autism Res, 2016. 9(7): p. 790-800.
Moriuchi, J.M., A. Klin, and W. Jones, Mechanisms of Diminished Attention to Eyes in Autism. Am J Psychiatry, 2016: p. appiajp201615091222.
Scahill, L., et al., Effect of Parent Training on Adaptive Behavior in Children With Autism Spectrum Disorder and Disruptive Behavior: Results of a Randomized Trial. J Am Acad Child Adolesc Psychiatry, 2016. 55(7): p. 602-609 e3.
Smith, T., et al., Atomoxetine and Parent Training for Children With Autism and Attention-Deficit/Hyperactivity Disorder: A 24-Week Extension Study. J Am Acad Child Adolesc Psychiatry, 2016. 55(10): p. 868-876 e2.
McKnight, L.M., M.P. O’Malley-Keighran, and C. Carroll, ‘Just wait then and see what he does’: a speech act analysis of healthcare professionals’ interaction coaching with parents of children with autism spectrum disorders. Int J Lang Commun Disord, 2016. 51(6): p. 757-768.
Ooi, Y.P., et al., Oxytocin and Autism Spectrum Disorders: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Pharmacopsychiatry, 2016.
Gordon, I., et al., Intranasal Oxytocin Enhances Connectivity in the Neural Circuitry Supporting Social Motivation and Social Perception in Children with Autism. Sci Rep, 2016. 6: p. 35054.
Hernandez, L.M., et al., Additive effects of oxytocin receptor gene polymorphisms on reward circuitry in youth with autism. Mol Psychiatry, 2016.
Westberg, L., et al., Variation in the Oxytocin Receptor Gene Is Associated with Face Recognition and its Neural Correlates. Front Behav Neurosci, 2016. 10: p. 178.
Watanabe, T., et al., Oxytocin receptor gene variations predict neural and behavioral response to oxytocin in autism. Soc Cogn Affect Neurosci, 2016.
Yang, D., et al., Brain responses to biological motion predict treatment outcome in young children with autism. Transl Psychiatry, 2016. 6(11): p. e948.
Mandell, D.S., et al., Effects of Autism Spectrum Disorder Insurance Mandates on the Treated Prevalence of Autism Spectrum Disorder. JAMA Pediatr, 2016. 170(9): p. 887-93.
Levy, S.E., et al., Shared Decision Making and Treatment Decisions for Young Children With Autism Spectrum Disorder.Acad Pediatr, 2016. 16(6): p. 571-8.
This year was filled with both challenges and encouraging signs of progress. The world continues to cope with the many hardships associated with the COVID-19 pandemic, which have negatively impacted the community, including scientists who study autism. Families and individuals continue to show individualized and specialized needs, specifically those from racially and ethnically diverse communities, females and girls, and we continue to understand the specific needs of those groups. For example, the close of the year saw the publication of a report by the Lancet Commission, which formally introduces the concept of “profound autism” representing individuals with different support needs. New CDC data released in December also show that autism rates are rising while age at diagnosis is decreasing [1]. While this is not a comprehensive summary of every single autism discovery in 2021, here we summarize many significant autism discoveries and related news of the past year:
Lancet Commission Endorses Use of Term “Profound Autism”
On December 6, The Lancet published an extensive report from a global team of autism researchers and stakeholders. The report, titled “The Lancet Commission on the Future of Care and Clinical Research in Autism,” recognized that effective autism assessment and care require personalized, stepped-care approaches that meet an individual’s needs throughout their lives, and that greater investment is urgently needed to develop and refine practical interventions that can improve the lives of people with autism. The Commission also formally introduced the term “profound autism” to distinguish individuals who have high dependency needs and urged policymakers to focus on the unique needs of this group, which represents approximately 30% of people with autism [2]. The goal of this label is to recognize the uniqueness of these individuals and that their support needs and outcomes are different from those of others. There is also evidence that the underlying biology of those with “profound autism” is different [3-5].
Amy and Jonah Lutz
The term “profound autism” is intended to describe autistic people who are likely to need 24-hour support throughout their lives. The report states that useful categories like “profound autism” can bring attention to the different needs of different people. In fact, the goal of the new term “profound autism” is to equip parents, service providers and the public with the language necessary to ensure that each individual with autism receives the accommodations and interventions they need [2]. These can vary greatly. Some of those diagnosed with autism engage in destructive or self-injurious behavior. Some have intellectual disabilities; others are star students. Some are unable to perform basic tasks like brushing their teeth and getting dressed; others can live fully independent lives. Autism is a disorder in which no two diagnoses look the same, and terms like “profound autism” help distinguish needs
CDC Reports Autism Prevalence Continues to Rise
The CDC ADDM Network released updated autism prevalence data this year, announcing that one in 44 8-year-old children is diagnosed with autism [1]. This is an increase from the one in 54 number for 8-year-olds reported in March 2020. Using a slightly different but validated methodology from previous years [6], new CDC data confirm that autism prevalence and diagnoses have gone up steadily in the past five years.
The CDC information makes it clear that we are getting better at diagnosing autism and identifying it earlier, which is encouraging because research has consistently shown the value of early intervention. However, more than 58% of children identified had intellectual disability or borderline intellectual disability. This cohort of children with profound autism warrants more attention from policymakers and service providers, as their needs are dramatically different from those with milder forms of autism. While the prevalence went up, the demographics across race, ethnicity and cognitive ability stayed pretty stable from the last prevalence estimate [1]. This information calls for further understanding of the nature of this rise beyond just diagnostic practices, including alerting pediatricians and supporting further and more expanded studies of gene x environment interactions [7]. One example would be the differential influence of toxic chemicals on cells with genetic mutations associated with autism, which revealed a susceptibility to toxic chemical exposures with cells with autism-related variation [8].
Reaching the Hard to Reach
Those from racially and ethnically diverse backgrounds have long been recognized as being diagnosed later, if at all. There are years and years of CDC data which show that while this trend is improving, it is still problematic in terms of equitable access to services. It also produces another problem that perpetuates the underdiagnosis and lack of access: not enough families from racially and ethnically diverse communities are being studied in research, which means most research findings apply to white communities, not the communities represented in the real world who need help [9]. A few studies this year specifically targeted those from either Hispanic [10] or Black and Hispanic families [11, 12]and found their needs were different or developed tools for their particular culture. However, in a commentary this year, researchers highlighted the need to engage diverse communities at the beginning of the research question, to ensure they have a voice at each step, and to possibly adapt the study question to their particular circumstances [9].
Donielle Johsnon with her family
Unfortunately, not all of the challenges facing underserved communities are the same. For example, those who are minimally verbal and have intellectual disabilities are left out of research for logistical reasons, or, in many cases, the intellectual and verbal abilities of individuals with more profound autism are not reported at all [13]. Those with intellectual disability are usually recognized more often, but there were only four intervention studies published in PubMed in 2021 that specifically included a group of autistic people with intellectual disability.
Understanding Autism in Females
While females with ASD have not typically been placed in the “underdiagnosed” category, they certainly are a group that has been underserved by scientific research. Because of the 4:1 difference in prevalence for males to females, autism research studies typically include four times fewer females, which means findings are not generalizable to females [14-17].
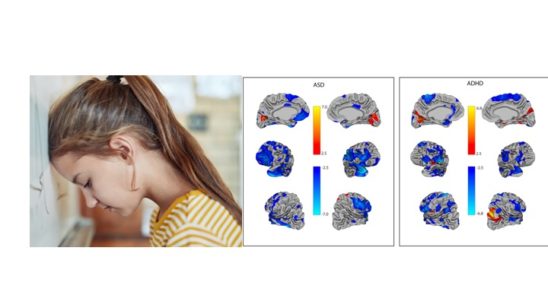
In the last year, there have been several studies showing that the challenges faced by autistic females are different from those facing autistic males. For example, a phenomenon called “passing as autistic” (otherwise known as masking) — where someone with autism tries to hide their symptoms to pass in social situations — was found to be elevated in females [18, 19]. Comorbidities like epilepsy have been shown to be higher in females [20], and baseline brain activity in autistic youth is different based on biological sex [16]. While the female brain is clearly different from the male brain, even in autism, the lack of females included in research has also significantly impaired our understanding of brain differences between males and females with ASD for more personalized support [21].
Because of the disparity in diagnosis between males and females, there are very few studies that can examine the effects of sex and gender on diagnosis, making consistent findings across sex/gender almost impossible, but it has been done [22]. What has been learned is that the striatum (and genes controlling striatal development) may play a role in autism symptoms in females. This has not been identified as an area of interest in males [23]. Research also shows that females have a higher burden of variants in the oxytocin receptor gene, which affect them differently than males with ASD [15], and differential links between brain activity and autism features [16], supporting something called the “female protective effect.” This protective effect might be genetic or might occur through the estrogen pathway [24, 25]. Finally, while the entire autism community has a higher than expected rate of gender dysphoria, it seems to affect girls more than boys [26]. Behavioral features are also slightly different, which complicates diagnosis [17]. Together, these results demonstrate that scientific findings, including use of biomarkers for diagnosis, which are seen in males may be different than those seen in females. Scientists need to ensure that enough females are recruited into research studies and better understand the difference between females and males to ensure that scientific findings generalize to care in the community.
The Pandemic Is Still Causing Problems
Almost two years into the pandemic, scientists are still working to understand the long-term effects on people with autism. Studies focused on increases in challenging behaviors and loneliness in autistic youth and adults [27, 28], and also on understanding the mental health challenges due to prolonged social distancing guidelines, including multiple waves of lockdowns [29-32]. Additionally, studies show that families with autism are disproportionately affected by job losses and food insecurity [33, 34]. And while telehealth-based diagnosis and services are becoming more common as a result of social distancing, families of younger children who need direct behavioral supports remain the least satisfied [35, 36], a trend continuing from 2020 [37]. The challenges associated with the pandemic are not limited to those with a diagnosis and their families. Scientists who dedicate their lives to help those on the spectrum have struggled with some of the same issues that families with autism have [38], including mental health and childcare challenges. This compounds the problem of developing scientific discoveries and delivering them to the community.
New Technologies for Diagnosis and Treatment
With the pandemic came the use of remote and virtual technologies, not just to identify and diagnose autism, but also to provide supports and services. As the pandemic continues, researchers are studying what works and what doesn’t, especially in families who say that they found telehealth more accessible and beneficial [35]. Remote assessments have changed the nature of how autism is diagnosed, with scientists emphasizing the need for use of good clinical judgment rather than reliance on singular instruments [39]. Telehealth assessments have meant that diagnosis is now more accessible to those in remote areas who are traditionally underdiagnosed. Another bright spot is that the pandemic has allowed children to be observed remotely in their home environment, which may significantly enhance the ability of clinicians to observe early markers of autism [39, 40]. New technologies that enable videotaping via remote camera — for later review by clinicians — are also gaining traction. Recently, Cognoa received FDA marketing authorization for its new remote videotaping tool, CanvasDx. Duke University also published data a tool that plays different movies and visual scenes on an iPad and allows clinicians to determine the likelihood of an autism diagnosis by examining where the children looked in the scene [41], as past research has shown that children with autism are more likely to look at objects and less likely to look at social stimuli. In both cases, these recordings, together with standard early screening methods, can be analyzed to help facilitate diagnosis. A 2021 review found these mobile digital technologies to be promising in diagnosis [42].
Beyond just supporting diagnosis, mobile technology may be used to improve cognitive and social skills across the lifespan [43]. A recent systematic review indicated that these mobile interventions were particularly helpful in targeting practical skills [43, 44]. They can also be used to predict responses to stressful situations and abnormal sensory arousal [45]. Finally, robots and videogames on devices are showing promise in helping kids with autism develop social skills [46, 47]. While these technologies may have benefits beyond the pandemic and can alleviate some of the burden of traveling to multiple appointments, they will not replace the need for children to be diagnosed and/or receive therapy from trained, in-person clinicians [39, 48].
Intervention Before Diagnosis
A few years ago, scientists in the UK began studying the possibility of promoting skills in parents as a way to mitigate autism symptoms in infants [49]. By working with parents in their home and promoting social and communication skills through activities like reading and play, autism severity scores improved. This year, a group in Australia conducted its own randomized controlled study starting at 9-12 months — before a diagnosis can be made — to provide support to parents and offer video feedback on supporting language and social development in their infants. This study showed that support of infant social and communication skills measured at one year led to a reduction of autism severity scores at 24 months, with these improvements being maintained long after the end of the intervention period [50]. Factors like caregiver interaction and adjusting the environment to promote learning in these toddlers are key ingredients to changing developmental trajectory [51, 52]. New tools are also allowing earlier and earlier detection of markers of ASD, with some evidence that it can be done as early as 12 months of age [53]. These findings represent the potential benefits of decades worth of early detection work and operationalize a methodology for parents to learn to promote social and communication skills in their infants.
However, the need for earlier detection and diagnosis of autism remains a priority within autism research and the autism community. This year, researchers identified changes in the grey matter (cell bodies) and white matter (the neuron branches) in children as young as 12 months of age [54] who go on to be diagnosed with autism. Changes in brain activity, while not a diagnostic marker, can be seen in infants as young as 3 months of age [55] and can prove helpful in diagnosis at 6 months [56]. In addition, some behavioral signs can also trigger preemptive intervention. Groups led by UC Davis demonstrated both declining gaze to faces, which was replicated in two different cohorts [57], and unusual inspection of objects at 9 months, which predicts reduced social engagement at 12 months in those who later develop an autism diagnosis [58]. In addition, vocalizations (or intents to communicate) were lower in children as young as 12 months [59]. Together, while not diagnostic, some of these early markers and signs can facilitate entry into preemptive interventions, which can produce skills in caregivers and infants that change the developmental trajectory. Finally, there is an erroneous perception that parents believe that all of autism is “bad” and needs to “be eliminated.” In fact, when they were specifically asked, parents identified characteristics like love, kindness, humor, humanity and resilience that they value and appreciate in their children [60].
Autism and Aging
There has traditionally been a lack of understanding as to what happens to autistic adults as they enter their golden years. This year, Drexel University utilized Medicaid data to examine the risk of dementia in those with autism and found that those with ASD were 2.6 times more likely to be diagnosed with dementia compared to the general population [61]. This has profound impacts on planning for elderly relatives with ASD and developing interventions that may stunt the development of dementia in this population.
Understanding the Role of Genetics in Autism
Traditionally, genetic variation association with autism has been bucketed as “rare” mutations and “common” mutations. Rare mutations on genes typically lead to deleterious effects such as seizures or intellectual disability [62]. Sometimes, like in the case of BRCA (breast cancer gene), they can be fatal. Common mutations are seen in lots of people, not just those with autism, but the human body can tolerate many common mutations with no major effects. However, if the genetic variant is found in an autism risk gene, for example, then it can dispose someone to an autism diagnosis [62]. Mutations found in autism risk genes — including those associated with cell adhesion, neuron-glia interactions and synapse formation — are most likely to be common variants involved in autism [3].
This year, sequencing of more than 800 people with an autism diagnosis revealed that 27% had evidence of a rare genetic mutation, mostly in one of the 102 genes identified in 2020 as being relevant for ASD [3, 63]. Presence of a mutation of one of these genes also results in a distinct set of behavioral features early in life that is different from those without a rare mutation [64]. Interestingly, instead of advancing the traditional “rare vs. common variation debate,” scientists this year learned that even in those who have a rare genetic mutation, there is also a high burden of common variation [63]. Scientists found that both rare and common genetic risks contribute to autism susceptibility, and that the dual risks may increase the likelihood of an autism diagnosis [63]. These findings make things complicated for genetic counselors who need to assess all the factors and communicate to families whether or not a particular rare variant is causative. In addition, sequencing technologies are revealing more and more genes that are relevant to ASD but incredibly rare; in fact, they are likely to be part of a multi-factorial cause of individual cases of ASD [65]. Finally, we’ve learned that common variation influences not only core autism symptoms, but also psychiatric comorbidities [66].
Studying Rare Genetic Syndromes Opens the Door to New Therapeutics
The use of induced pluripotent stem cells, or iPSCs, to study the brain on a cellular level has so far been focused on rare genetic diseases associated with autism, like Dup15q syndrome, CNTNAP2 and CDKL5 disorder. However, while the genetic targets may be more specific than in idiopathic autism, there are also converging mechanisms of disrupted connectivity in the brain that make these single gene disorders useful in understanding the neurobiology of ASD [67-71].
In addition to some shared (and some distinct) neurobiology across autism with a known genetic cause, there is overlap on the basic neurobiology level in terms of cortical thickness [72] and G-protein-coupled-receptors across different psychiatric disorders, including autism [73]. Some of these rare genetic syndromes have been responsive to targeted gene therapy, which opens up the door for them to be used in idiopathic autism if proven safe and effective in large groups of people with neurodevelopmental disorders.
Remember Glial Cells? They May Play a Bigger Role Than We Thought.
One brain cell type that is experiencing renewed interest in autism is glial cells, particularly with regard to sex differences in ASD. Glial cells are found in the brain, but they do not communicate with each other. Rather, they provide insulation to neurons that do communicate via electrical impulses. Traditionally, because they were not thought to be communication cells, they were not considered critical for study. But recent evidence has shown that there may be different subtypes of autism defined by the upregulation of genes that control glial cells [74]. Gene expression in these microglia may also contribute to differences in brain structure [75]. In addition, the direct study of brain tissue has shown that in certain layers of the cortex, astrocytes — a type of glial cell — are decreased [76]. Taken together, the dysregulation of glial cells may contribute to different cell processes, brain structure, functional changes and psychiatric syndromes associated with autism.
What Can We Do to Improve Outcomes of Those with Autism?
New research shared this year focused on improving outcomes. First, we learned that the presence of a brother or sister not on the autism spectrum improves adaptive behavior across the lifespan for those with an autism diagnosis [77]. On the other hand, parental stress in early life and early adverse events can make outcomes worse [78].
Research continues to show that, especially in the early years, parents and caregivers can play a critical and life-changing role in their child’s development. For young children, Naturalistic Developmental Behavioral Interventions (NDBIs), which are child-led and utilize behavioral principles delivered in the home, are most helpful [79, 80] and now may be delivered via telehealth [81]. One good thing to come out of the pandemic is the availability ofremote access to video series, including but not limited to the Autism Navigator, which can help parents identify early signs and deliver these interventions to their young children from home [82]. The literature on the efficacy of these NDBIs grows greater every year. However, not everyone has access to early interventions or even expert clinicians. To address the disparities seen across the world and across different comorbidities and other individual factors, the Lancet Commission report called for a stepped-care and personalized health model for interventions [2]. This includes provisions not just for individual and family factors, but also for accessibility and cost. These recommendations on how different groups approach care are essential to obtain a more specialized approach to helping families and individuals on the spectrum lead happy, healthy and successful lives. Unfortunately, some promising therapeutics like oxytocin failed to meet the cut of significantly helping those with ASD [83]. Other organ systems besides the brain, including the gastrointestinal system, continue to be investigated to help alleviate co-occurring medical conditions. Many families turn to things like probiotics to help with issues like constipation and diarrhea, however, new evidence suggests that the microbiome is more influenced by diet than autism itself [84] calling into question the validity of probiotic use for GI problems.
In Memoriam
Sadly, the autism community lost three scientists this year who have made enormous contributions to the field and changed the way people think about autism. Sir Michael Rutter, known as the Father of Child Psychiatry, a professor at the Institute of Psychiatry at Kings College London, was one of the most influential psychiatric scientists of the past 50 years. He was one of the first researchers to study autism, publishing a study of autistic twins in 1977. He helped dispel the myth that parenting styles influenced an autism diagnosis and brought scientific rigor to understanding autism. He helped develop the two gold standard tools for diagnosis: the ADI-R and the ADOS. His commitment to helping children and families was not limited to autism, however; he helped families with a number of psychiatric conditions and behavioral issues.
Li-Ching Lee, who served as the Associate Director for Global Autism at the Wendy Klag Center of Johns Hopkins School of Public Health, was one of the reasons why autism is recognized as a global condition. She focused her research on identifying and helping families with autism across the world, calling it a “human rights issue” when the needs of families in under-resourced countries were ignored. She also worked tirelessly to understand autism in the US, working closely with the CDC to understand who and where people were being diagnosed and how they could be helped. Beyond being an amazing scientist, her fellow students have called her an amazing friend, mentor and teacher who went above and beyond to help her students be successful while helping families.
Finally, George C. Wagner of Rutgers University was one of the first behavioral neuroscientists to try to develop a behavioral model of ASD in rodents at a time when scientists were starting to try to understand how to recapitulate the features in model systems. His work helped define how autism should be studied in animals, and how it overlapped or was different than other psychiatric disorders. He based his models on the core features rather than particular behaviors, including delay of skill development, plateauing of skills and possible regression of skills. This helped fundamentally change the field of animal models of ASD. Many of his students (including ASF CSO Alycia Halladay) went on to help families with ASD following training.
All three of these amazing scientists will be remembered not just for their contributions to science, but for their training of early career researchers who continue to make an impact.
The Last Word
Over the last 40 years, autism has moved from a categorial (yes/no) diagnosis to a dimensional diagnosis [85], taking into account the complexity and differences of features across the lifespan. While there may be core features of ASD that are common across the spectrum, people with autism, just like people without autism, are all different and need to be recognized as such [2, 86].
While this summary captures what happened in 2021, we urge you to read more about how science has changed the way families with autism have been perceived, treated and helped over the past 40 years. The Journal of Autism and Developmental Disorderspublished a series that you can look through here, and Dr. Giacomo Vivanti shared his long-term perspective on the November 14 ASF podcast here: https://asfpodcast.org/archives/1258. In fact, one of the best ways to keep up with changes in autism science is to subscribe to the ASF podcast on Spotify, Apple Podcasts or Google Podcasts.
You can make a difference
These research findings and important discoveries were thanks to the thousands of families and autistic individuals who participated in research studies over the past few years. As you can read from this report, your contributions make an impact. There are other research opportunities and as we continue to live in the pandemic, many more of them are available in your own home with interaction with professionals to support you. You can read more about them here. Finally, there are ways to learn about credible science outside social media, which also includes SpectrumNews and the Autism BrainNet. Just signing up for more information on the Autism BrainNet gets you regular information about what the brains of autistic people look like and how they are different from those without a diagnosis.
References
1. Maenner, M.J., et al., Prevalence and Characteristics of Autism Spectrum Disorder Among Children Aged 8 Years – Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2018. MMWR Surveill Summ, 2021. 70(11): p. 1-16.
2. Lord, C., et al., The Lancet Commission on the future of care and clinical research in autism. The Lancet, 2021.
3. Mahjani, B., et al., Prevalence and phenotypic impact of rare potentially damaging variants in autism spectrum disorder. Mol Autism, 2021. 12(1): p. 65.
4. Havdahl, A., et al., Age of walking and intellectual ability in autism spectrum disorder and other neurodevelopmental disorders: a population-based study. J Child Psychol Psychiatry, 2021. 62(9): p. 1070-1078.
5. Reardon, A.M., et al., Subtyping Autism Spectrum Disorder Via Joint Modeling of Clinical and Connectomic Profiles. Brain Connect, 2021.
6. Maenner, M.J., et al., Comparison of 2 Case Definitions for Ascertaining the Prevalence of Autism Spectrum Disorder Among 8-Year-Old Children. Am J Epidemiol, 2021. 190(10): p. 2198-2207.
7. Volk, H.E., et al., Considering Toxic Chemicals in the Etiology of Autism. Pediatrics, 2021.
8. Modafferi, S., et al., Gene-Environment Interactions in Developmental Neurotoxicity: a Case Study of Synergy between Chlorpyrifos and CHD8 Knockout in Human BrainSpheres. Environ Health Perspect, 2021. 129(7): p. 77001.
9. Maye, M., et al., Biases, Barriers, and Possible Solutions: Steps Towards Addressing Autism Researchers Under-Engagement with Racially, Ethnically, and Socioeconomically Diverse Communities. J Autism Dev Disord, 2021.
10. Harris, J.F., et al., Validation of the Developmental Check-In Tool for Low-Literacy Autism Screening.Pediatrics, 2021. 147(1).
11. Azad, G., et al., The influence of race on parental beliefs and concerns during an autism diagnosis: A mixed-method analysis. Autism, 2021: p. 13623613211044345.
12. Wagner, S., I.L. Rubin, and J.S. Singh, Underserved and Undermeasured: a Mixed-Method Analysis of Family-Centered Care and Care Coordination for Low-Income Minority Families of Children with Autism Spectrum Disorder. J Racial Ethn Health Disparities, 2021.
13. Thurm, A., et al., Making Research Possible: Barriers and Solutions For Those With ASD and ID. J Autism Dev Disord, 2021.
14. Skaletski, E.C., et al., Quality-of-Life Discrepancies Among Autistic Adolescents and Adults: A Rapid Review. Am J Occup Ther, 2021. 75(3).
15. Lawrence, K.E., et al., Impact of autism genetic risk on brain connectivity: a mechanism for the female protective effect. Brain, 2021.
16. Neuhaus, E., et al., Resting state EEG in youth with ASD: age, sex, and relation to phenotype. J Neurodev Disord, 2021. 13(1): p. 33.
17. Dillon, E.F., et al., Sex Differences in Autism: Examining Intrinsic and Extrinsic Factors in Children and Adolescents Enrolled in a National ASD Cohort. J Autism Dev Disord, 2021.
18. Libsack, E.J., et al., A Systematic Review of Passing as Non-autistic in Autism Spectrum Disorder. Clin Child Fam Psychol Rev, 2021. 24(4): p. 783-812.
19. Cook, J., et al., Camouflaging in autism: A systematic review. Clin Psychol Rev, 2021. 89: p. 102080.
20. Bougeard, C., et al., Prevalence of Autism Spectrum Disorder and Co-morbidities in Children and Adolescents: A Systematic Literature Review. Front Psychiatry, 2021. 12: p. 744709.
21. Mo, K., et al., Sex/gender differences in the human autistic brains: A systematic review of 20 years of neuroimaging research. Neuroimage Clin, 2021. 32: p. 102811.
22. Floris, D.L., et al., Towards robust and replicable sex differences in the intrinsic brain function of autism. Mol Autism, 2021. 12(1): p. 19.
23. Jack, A., et al., A neurogenetic analysis of female autism. Brain, 2021. 144(6): p. 1911-1926.
24. Enriquez, K.D., A.R. Gupta, and E.J. Hoffman, Signaling Pathways and Sex Differential Processes in Autism Spectrum Disorder. Front Psychiatry, 2021. 12: p. 716673.
25. Willsey, H.R., et al., Parallel in vivo analysis of large-effect autism genes implicates cortical neurogenesis and estrogen in risk and resilience. Neuron, 2021. 109(5): p. 788-804 e8.
26. Brunissen, L., et al., Sex Differences in Gender-Diverse Expressions and Identities among Youth with Autism Spectrum Disorder. Autism Res, 2021. 14(1): p. 143-155.
27. Hards, E., et al., Loneliness and mental health in children and adolescents with pre-existing mental health problems: A rapid systematic review. Br J Clin Psychol, 2021.
28. Kalb, L.G., et al., Psychological distress among caregivers raising a child with autism spectrum disorder during the COVID-19 pandemic. Autism Res, 2021. 14(10): p. 2183-2188.
29. Young, E., et al., Caregiver burnout, gaps in care, and COVID-19: Effects on families of youth with autism and intellectual disability. Can Fam Physician, 2021. 67(7): p. 506-508.
30. Polonyiova, K., et al., Comparing the impact of the first and second wave of COVID-19 lockdown on Slovak families with typically developing children and children with autism spectrum disorder. Autism, 2021: p. 13623613211051480.
31. Siracusano, M., et al., Parental Stress and Disability in Offspring: A Snapshot during the COVID-19 Pandemic. Brain Sci, 2021. 11(8).
32. Lois Mosquera, M., et al., Autistic adults’ personal experiences of navigating a social world prior to and during Covid-19 lockdown in Spain. Res Dev Disabil, 2021. 117: p. 104057.
33. Karpur, A., et al., Food insecurity in the households of children with autism spectrum disorders and intellectual disabilities in the United States: Analysis of the National Survey of Children’s Health Data 2016-2018. Autism, 2021. 25(8): p. 2400-2411.
34. Panjwani, A.A., R.L. Bailey, and B.L. Kelleher, COVID-19 and Food-Related Outcomes in Children with Autism Spectrum Disorder: Disparities by Income and Food Security Status. Curr Dev Nutr, 2021. 5(9): p. nzab112.
35. Bhat, A., Analysis of the SPARK study COVID-19 parent survey: Early impact of the pandemic on access to services, child/parent mental health, and benefits of online services. Autism Res, 2021. 14(11): p. 2454-2470.
36. Corona, L.L., et al., Utilization of telemedicine to support caregivers of young children with ASD and their Part C service providers: a comparison of intervention outcomes across three models of service delivery. J Neurodev Disord, 2021. 13(1): p. 38.
37. Jeste, S., et al., Changes in access to educational and healthcare services for individuals with intellectual and developmental disabilities during COVID-19 restrictions. J Intellect Disabil Res, 2020.
38. Harrop, C., et al., A lost generation? The impact of the COVID-19 pandemic on early career ASD researchers. Autism Res, 2021. 14(6): p. 1078-1087.
39. Zwaigenbaum, L., et al., Rethinking autism spectrum disorder assessment for children during COVID-19 and beyond. Autism Res, 2021. 14(11): p. 2251-2259.
40. Delehanty, A.D. and A.M. Wetherby, Rate of Communicative Gestures and Developmental Outcomes in Toddlers With and Without Autism Spectrum Disorder During a Home Observation. Am J Speech Lang Pathol, 2021. 30(2): p. 649-662.
41. Chang, Z., et al., Computational Methods to Measure Patterns of Gaze in Toddlers With Autism Spectrum Disorder. JAMA Pediatr, 2021. 175(8): p. 827-836.
42. Desideri, L., P. Perez-Fuster, and G. Herrera, Information and Communication Technologies to Support Early Screening of Autism Spectrum Disorder: A Systematic Review. Children (Basel), 2021. 8(2).
43. de Nocker, Y.L. and C.K. Toolan, Using Telehealth to Provide Interventions for Children with ASD: a Systematic Review. Rev J Autism Dev Disord, 2021: p. 1-31.
44. Leung, P.W.S., et al., Effectiveness of Using Mobile Technology to Improve Cognitive and Social Skills Among Individuals With Autism Spectrum Disorder: Systematic Literature Review. JMIR Ment Health, 2021. 8(9): p. e20892.
45. Nuske, H.J., et al., Evaluating commercially available wireless cardiovascular monitors for measuring and transmitting real-time physiological responses in children with autism. Autism Res, 2021.
46. Penev, Y., et al., A Mobile Game Platform for Improving Social Communication in Children with Autism: A Feasibility Study. Appl Clin Inform, 2021. 12(5): p. 1030-1040.
47. Riches, S., et al., Therapeutic engagement in robot-assisted psychological interventions: A systematic review. Clin Psychol Psychother, 2021.
48. Nuske, H.J. and D.S. Mandell, Digital health should augment (not replace) autism treatment providers.Autism, 2021. 25(7): p. 1825-1827.
49. Green, J., et al., Randomised trial of a parent-mediated intervention for infants at high risk for autism: longitudinal outcomes to age 3 years. J Child Psychol Psychiatry, 2017. 58(12): p. 1330-1340.
50. Whitehouse, A.J.O., et al., Effect of Preemptive Intervention on Developmental Outcomes Among Infants Showing Early Signs of Autism: A Randomized Clinical Trial of Outcomes to Diagnosis. JAMA Pediatr, 2021. 175(11): p. e213298.
51. Davis, P.H., et al., Caregiver responsiveness as a mechanism to improve social communication in toddlers: Secondary analysis of a randomized controlled trial. Autism Res, 2021.
52. Grzadzinski, R., et al., Pre-symptomatic intervention for autism spectrum disorder (ASD): defining a research agenda. J Neurodev Disord, 2021. 13(1): p. 49.
53. Wetherby, A.M., et al., The Early Screening for Autism and Communication Disorders: Field-testing an autism-specific screening tool for children 12 to 36 months of age. Autism, 2021. 25(7): p. 2112-2123.
54. Godel, M., et al., Altered Gray-White Matter Boundary Contrast in Toddlers at Risk for Autism Relates to Later Diagnosis of Autism Spectrum Disorder. Front Neurosci, 2021. 15: p. 669194.
55. Tran, X.A., et al., Functional connectivity during language processing in 3-month-old infants at familial risk for autism spectrum disorder. Eur J Neurosci, 2021. 53(5): p. 1621-1637.
56. Peck, F.C., et al., Prediction of autism spectrum disorder diagnosis using nonlinear measures of language-related EEG at 6 and 12 months. J Neurodev Disord, 2021. 13(1): p. 57.
57. Gangi, D.N., et al., Declining Gaze to Faces in Infants Developing Autism Spectrum Disorder: Evidence From Two Independent Cohorts. Child Dev, 2021. 92(3): p. e285-e295.
58. Miller, M., et al., Repetitive behavior with objects in infants developing autism predicts diagnosis and later social behavior as early as 9 months. J Abnorm Psychol, 2021. 130(6): p. 665-675.
59. Plate, S., et al., Infant vocalizing and phenotypic outcomes in autism: Evidence from the first 2 years. Child Dev, 2021.
60. Cost, K.T., et al., “Best Things”: Parents Describe Their Children with Autism Spectrum Disorder Over Time.J Autism Dev Disord, 2021. 51(12): p. 4560-4574.
61. Vivanti, G., et al., The prevalence and incidence of early-onset dementia among adults with autism spectrum disorder. Autism Res, 2021. 14(10): p. 2189-2199.
62. Gaugler, T., et al., Most genetic risk for autism resides with common variation. Nat Genet, 2014. 46(8): p. 881-5.
63. Klei, L., et al., How rare and common risk variation jointly affect liability for autism spectrum disorder. Mol Autism, 2021. 12(1): p. 66.
64. Wickstrom, J., et al., Patterns of delay in early gross motor and expressive language milestone attainment in probands with genetic conditions versus idiopathic ASD from SFARI registries. J Child Psychol Psychiatry, 2021. 62(11): p. 1297-1307.
65. Wilfert, A.B., et al., Recent ultra-rare inherited variants implicate new autism candidate risk genes. Nat Genet, 2021. 53(8): p. 1125-1134.
66. Rodriguez-Gomez, D.A., et al., A systematic review of common genetic variation and biological pathways in autism spectrum disorder. BMC Neurosci, 2021. 22(1): p. 60.
67. de Jong, J.O., et al., Cortical overgrowth in a preclinical forebrain organoid model of CNTNAP2-associated autism spectrum disorder. Nat Commun, 2021. 12(1): p. 4087.
68. Jacot-Descombes, S., et al., Altered synaptic ultrastructure in the prefrontal cortex of Shank3-deficient rats.Mol Autism, 2020. 11(1): p. 89.
69. Colombo, E., et al., The K63 deubiquitinase CYLD modulates autism-like behaviors and hippocampal plasticity by regulating autophagy and mTOR signaling. Proc Natl Acad Sci U S A, 2021. 118(47).
70. Victor, A.K., et al., Molecular Changes in Prader-Willi Syndrome Neurons Reveals Clues About Increased Autism Susceptibility. Front Mol Neurosci, 2021. 14: p. 747855.
71. Vasic, V., et al., Translating the Role of mTOR- and RAS-Associated Signalopathies in Autism Spectrum Disorder: Models, Mechanisms and Treatment. Genes (Basel), 2021. 12(11).
72. Writing Committee for the Attention-Deficit/Hyperactivity, D., et al., Virtual Histology of Cortical Thickness and Shared Neurobiology in 6 Psychiatric Disorders. JAMA Psychiatry, 2021. 78(1): p. 47-63.
73. Monfared, R.V., et al., Transcriptome Profiling of Dysregulated GPCRs Reveals Overlapping Patterns across Psychiatric Disorders and Age-Disease Interactions. Cells, 2021. 10(11): p. 2967.
74. Nassir, N., et al., Single-cell transcriptome identifies molecular subtype of autism spectrum disorder impacted by de novo loss-of-function variants regulating glial cells. Hum Genomics, 2021. 15(1): p. 68.
75. Takanezawa, Y., et al., Microglial ASD-related genes are involved in oligodendrocyte differentiation. Sci Rep, 2021. 11(1): p. 17825.
76. Falcone, C., et al., Neuronal and glial cell number is altered in a cortical layer-specific manner in autism.Autism, 2021. 25(8): p. 2238-2253.
77. Rosen, N.E., J.B. McCauley, and C. Lord, Influence of siblings on adaptive behavior trajectories in autism spectrum disorder. Autism, 2021: p. 13623613211024096.
78. Hollocks, M.J., et al., The association of adverse life events and parental mental health with emotional and behavioral outcomes in young adults with autism spectrum disorder. Autism Res, 2021. 14(8): p. 1724-1735.
79. Schuck, R.K., et al., Neurodiversity and Autism Intervention: Reconciling Perspectives Through a Naturalistic Developmental Behavioral Intervention Framework. J Autism Dev Disord, 2021.
80. Waddington, H., et al., The effects of JASPER intervention for children with autism spectrum disorder: A systematic review. Autism, 2021. 25(8): p. 2370-2385.
81. Dai, Y.G., et al., Development and Acceptability of a New Program for Caregivers of Children with Autism Spectrum Disorder: Online Parent Training in Early Behavioral Intervention. J Autism Dev Disord, 2021. 51(11): p. 4166-4185.
82. Wainer, A.L., et al., Examining a stepped-care telehealth program for parents of young children with autism: a proof-of-concept trial. Mol Autism, 2021. 12(1): p. 32.
83. Sikich, L., et al., Intranasal Oxytocin in Children and Adolescents with Autism Spectrum Disorder. N Engl J Med, 2021. 385(16): p. 1462-1473.
84. Yap, C.X., et al., Autism-related dietary preferences mediate autism-gut microbiome associations. Cell, 2021. 184(24): p. 5916-5931 e17.
85. Rosen, N.E., C. Lord, and F.R. Volkmar, The Diagnosis of Autism: From Kanner to DSM-III to DSM-5 and Beyond. J Autism Dev Disord, 2021. 51(12): p. 4253-4270.
86. Lord, C. and S.L. Bishop, Let’s Be Clear That “Autism Spectrum Disorder Symptoms” Are Not Always Related to Autism Spectrum Disorder. Am J Psychiatry, 2021. 178(8): p. 680-682.
A Summary of Autism Research in 2017 and What It Means for Families
By Alycia Halladay, PhD, Chief Science Officer of the Autism Science Foundation and the Scientific Advisory Board of the Autism Science Foundation
To listen to our year-end science summary podcast, click here.
This was not the first year that understanding the different subtypes of autism became a hot topic of discussion in the autism community, but in 2017, it certainly had much higher visibility on community blogs, in public speeches, editorials, science surveys, and public forums. There was especially fierce debate on the specific needs of people on the spectrum across the lifespan, with some divergence on the priorities of research.
The US Government Makes a Plan
Generating some of this discussion was the new strategic plan of the Interagency Autism Coordinating Committee (IACC). The committee, which is authorized by the Autism Cares Act, reconvened in 2015, but began work on a strategic plan for science this year. The IACC is made up of both public and private members representing funding agencies, advocacy organizations, people with autism, service providers, parents, and researchers, all members of the autism community. The group provides advice to the Secretary of Health and Human Services, collecting information from a wide variety of audiences to identify top priorities and needs in autism research. Importantly, the IACC does not make funding decisions, but the federal government uses its recommendations as a guide for calls for funding and other funding opportunities1.
Credit: National Institutes of Health
The IACC also writes a strategic plan for autism research each year, which guides but does not mandate funding opportunities. An updated IACC strategic plan published this year, reformulated seven crucial questions of importance for the autism community. It included an entire chapter devoted to meeting the needs of individuals as they move into adulthood, clearly an understudied and underfunded topic. The revision and expansion of this chapter sparked debate on what precisely those needs are.
Different Perspectives and Priorities
Surveys and interviews in the United Kingdom have revealed differences in the research priorities of different stakeholder groups2,3, and this year Autism Speaks conducted an online survey of its own4 which showed somewhat similar findings. As a whole, self-advocates and autistic adults place less of a priority on understanding early symptoms, biological mechanisms, causes, and treatments than parents. In addition to more formal findings in scientific literature, voices expressed via the blogosphere revealed highly disparate opinions of self-advocates5 and parents6. These differences may be partially explained by the differing abilities and disabilities of adults who are able to express their needs and voice their opinions and those who rely on parents or caregivers to do so.
But what does the science say? Qualitative research has revealed that autistic adults feel that research directed at changing them is counterproductive, and that adaptation needs to occur in the world around them3. Understandably, research priorities are also driven by individual personal experiences with individuals with autism and autistic adults7,8. While the goal of the DSM 5 was to provide a more accurate and specific diagnosis, an unintended consequence has been to lump the differently able autism groups into one definition, sometimes creating confusion and resentment when limited research money is involved.
Unfortunately, developing specific ways to distinguish the different subtypes of autism across the spectrum has proven elusive and remains one of the big challenges of autism researchers. Current large-scale research projects are focused on using biological approaches to distinguish the different subtypes. The subtypes will be used to understanding the different causes, to understand different strengths and abilities along with needs and disabilities, and to develop more focused, personalized treatments. These subtypes may be based on how individuals function in society.
This year, given new initiatives in sharing, pooling and standardizing larger data sets, researchers were able to re-examine the differences in autism phenotype, called the “autismS,” scientifically. The goal of identifying different subgroups of individuals with autism and autistic adults is to better characterize their needs and abilities toward tailoring services and supports, because the needs of each person can be so drastically different across the spectrum.
The Big Way the Ends of the Spectrum Are Different From Each Other
One factor that discerns both those who are able to self-advocate and those who need ongoing lifetime care is cognitive ability, measured by intellectual quotient or IQ. To truly understand the variability of people across the autism spectrum, big data is going to lead scientists to more answers.
This year, scientific research articles examined the different outcomes of individuals with autism with a wide range of cognitive abilities and found that IQ was an important predictor of outcomes in children with autism9-12. These included children involved in treatment studies as well as research cohorts. This is not necessarily a new finding, but it does replicate findings in larger cohorts that had previously only been replicated in smaller studies.
In these studies, autism severity scores, adaptive behaviors, and communication improved in individuals with higher IQs12; those with lower IQs typically had the highest severity symptoms10. Additionally, while stability of an autism diagnosis is high, children with autism who did ultimately move off the spectrum after diagnosis were more likely to have an average developmental quotient, reflecting higher cognitive ability13. Of course, early intellectual quotient does not fully explain outcome11, as language ability is also crucial12. It is also important to note that although cognition is often intact in individuals with optimal outcome, IQ alone does not always result in independent functioning. In other words, IQ is not the be-all-end-all of outcome in autism. As revealed in the Autism Speaks Autism Treatment Network, many individuals with ASD who do not have cognitive impairment exhibit significant deficits in adaptive functioning, and this gap has again been found to be larger in older versus younger individuals14. These differences can be associated with psychiatric comorbidities into adulthood15. These findings highlight the need for evaluating, monitoring, and treating adaptive behavior over time to determine whether an individual is independently applying her repertoire of cognitive skills to daily routines and activities when life demands them. The most comprehensive measure for assessing adaptive behavior is the Vineland Adaptive Behavior Scales, now in its Third Edition16, which helps clinicians better assess the role of adaptive behavior in both symptoms and a multitude of outcomes associated with autism.
Other larger scale studies to subtype children with autism have revealed that more subtle language use and language impairments do a good job of distinguishing different groups of people with autism, and that these groups also differ in non-verbal IQ17. In the Study to Explore Early Development, a project that included almost a thousand preschool children with autism, clinician scientists explored how symptoms cluster together to form groups, which may be then used to describe subtypes. Factors such as language impairments and cognitive rigidity predicted who was in what subtype18. This is the largest study so far to look at different aspects of functioning and abilities in a group of children with the intention of trying to group them into different types.
Beyond “Yes or No” as a Diagnosis
But why look at an autism diagnosis as an either/or thing when there is so much that distinguishes people across the spectrum? Rather than considering autism a “yes or no” diagnosis, there is now more evidence from larger groups that there are different dimensions of autism symptoms in children, including language and cognitive ability18. It is less about presence or absence of intellectual disability and language, but language and cognitive abilities along a continuum of impairment. Cognitive ability may also play a large role in autism diagnosis. A recent prospective study of the DSM-5 reinforced the high sensitivity and specificity of the newer DSM-5 criteria, while also revealing that those with higher IQ who were labeled under DSM-IV may not have met the threshold for an autism diagnosis under the DSM-519. Taken together, these studies further add to the research published this year that demonstrate different features of autism may constitute different types of autism, or new forms of autism altogether.
Efficacy of different intervention strategies also seems to be dependent on IQ of the child, as a scientific analysis of the anecdotal reports of fever improving symptoms was investigated. Parents with a child with lower non-verbal IQ and lower language levels reported more fever-related improvements in communication and repetitive behaviors20. This could be explained by multiple factors, including the presence of a definable subtype that is more responsive to different interventions.
The Biology Behind Autism Subtypes
Credit: Susanna M. Hamilton, courtesy of Broad Institute
Large-scale genetics studies of thousands of individuals with autism showed that different autism subtypes also have distinct genetic profiles. For example, those with what is known as a de novo mutation (not present in mother or father), show lower IQ scores and higher rates of epilepsy than those with what are known as common variants21. Therefore, different types of genetic mutations can have different influences on autism symptoms and can work together to shape different features of autism. Common variants, which can be inherited, are seen in everyone, but add together to increase risk of certain diseases like Alzheimer’s and Crohn’s. They do not seem to influence intellectual function in autism, while de novo variants do21. Whole genome sequencing studies also showed the diversity of different types of genetic variants in people with autism.22 While the association of de novo variants with lower IQ in individuals with autism is not a novel finding, the replication across multiple large-scale studies is an important contribution.
Adding to the complexity of the role of these de novo mutations, researchers discovered that when those with and without de novo mutations were matched based on IQ, those with de novo mutations actually have less pronounced autism symptoms23. Therefore, these finding suggest that these mutations may not confer any more risk for autism than other types of mutations. In other words, they may be more indicative of IQ than they are of autism. In addition, those individuals with de novo mutations had a different pattern of brain activity when shown non-social vs. social video scenes, independent of cognitive ability24. In fact, in some analyses, for people with autism and de novo gene mutations, intellectual disability is treated as a co-morbid symptom rather than a subtyping measure25. This again shows the differential influence of de novo gene mutations and other types of mutations on autism symptoms, and the importance of taking IQ into account when understanding autism and that presence of intellectual disability, presence of de novo variants, or both, may be a distinct autism subtype.
Big data, or large sample sizes, also helped scientists understand how an autism diagnosis influences immune functioning on a genetic level26 and has helped resolve discrepancies in findings in brain structure across studies. In fact, the largest study to date of people with autism at different ages illustrated that the cortex is most enlarged in adolescence, and replicated findings that other areas like the nucleus accumbens (moderating reward) and the amygdala (controlling emotion and anxiety) were smaller in those with autism27. The ultimate in “big data,” whole-genome sequencing, revealed new genes of interest and greater appreciation for the role of these genes. For example, one group found that previously understood areas of the genome, previously unstudied, could be important for ~6% of autism diagnoses22.
Presence of mutations in newly identified autism risk genes were also associated with lower adaptive ability, furthering the notion of a more severe genetic phenotype, as suggested earlier28.
With new datasets, it is also possible to determine the origin of when the de novo mutation occurred. As these de novo mutations occur in a small percentage of people with autism, large numbers are needed to better understand their influence and role in diagnosis. These different types of mutations can occur prior to the formation of the embryo, or in the post-zygotic period after the formation of the embryo. The timing of these mutations seems to have influence over behavioral features24 and has also been linked to the development of specific brain regions, specifically the amygdala29. There is also preliminary evidence to suggest that individuals with these post-zygotic mutations are less likely to be intellectually impaired29, again tying genetics with intellectual function and autism diagnosis. These post-zygotic mutations are present in a significant percentage of individuals with autism30, making them a potential target for new personalized medicine initiatives.
Genetics Provides More Answers
The genetic influence on specific behaviors, particularly autism-related behaviors, was better understood this year. By looking at twins, researchers were better able to establish the genetic influence of specific autism behaviors, specifically different eye gaze, which describes how people with autism pay more attention to objects and less to social situations31. This behavior controls how people with autism take in information about the world around them. Under strong genetic influence, eye gaze is altered in people with autism, and this differential input of different exposures then influences brain development. As Warren Jones, an author or the study stated, the effects of genetic influence on behavior “ripple forward” to alter brain development.
Genetics have also helped explain the comorbidity of autism with psychiatric issues and disorders. While behavioral overlap is seen between autism and disorders like schizophrenia, ADHD and anxiety, there have been few studies that identify a genetic overlap. This year, a novel locus on chromosome 10 was identified through large scale collaboration of multiple genetic cohorts32. With regards to schizophrenia, the exact symptoms and the mechanisms of schizophrenia and autism are not identical. But what causes the difference? To investigate, researchers used a sample of over 5000 individuals to determine the overlap between social communication symptoms in both autism and schizophrenia. It seems as the genetic influences of social communication features in autism and schizophrenia may be based on development, with one genetic factor being more prominent in early development (autism) and the other in adolescence (schizophrenia)33.
Credit: FamilieSCN2a Foundation
Beyond psychiatric comorbidities associated with autism, one of the concerns of both families and autistic adults is presence of medical comorbidities, such as epilepsy. A large percentage of people with autism have some form of epilepsy, but not everyone with epilepsy has autism. So is there something different about epilepsy in people with autism? In order to address this, scientists focused on the SCN2A gene, which codes for a sodium channel that can mediate the activity of a neuron34. Research using genetic, molecular and electrophysiological data showed that very tiny variations in the way this channel works may be at the center of these differences. Some mutations in the way the sodium channel functions are associated with epilepsy in the absence of autism, another type of mutation on this same gene which controls the same sodium channel is associated with epilepsy as a comorbid disorder to autism34. This opens up possibilities to both better understand autism and epilepsy, and how to treat the specific features of epilepsy in people with autism.
Other major breakthroughs were made using animal models to understand the molecular underpinnings of autism, providing new hope for novel drug treatments. For example, individuals with mutations of a specific region of chromosome 16 have a high risk of autism. A better understanding of genes on this chromosome could lead to more targeted treatments. One of these genes, KCTD13, was found to be crucial to the changes in synaptic plasticity associated with mutations of chromosome 16, and most importantly, these changes were reversed with a compound that inhibits a chemical called RhoA35. In another study, behavioral features following a particular mutation in the tuberous sclerosis gene in mice was shown to be similar to those with autism. These features were controlled by a particular cerebellar circuit, one that could be turned on and off in the animal model36 and rescued some of the behavioral features. Taken together, these exciting findings illustrate the capacity for new medical or pharmacological interventions to treat not all of autism, but particular symptoms determined in part, by the presence of different genetic mutations.
It’s Not All Just Genetics
Genetics is not the entire story in autism, and scientists continue to identify environmental factors that work together with genetics to confer risk, and through that, to identify ways to preempt symptoms, especially in those most disabled. In 2012, the first study appeared suggesting that maternal consumption of folic acid prior to pregnancy and during pregnancy reduced the probability of having a child diagnosed with autism. This year, two new large epidemiological studies in the US and Europe replicated and expanded these findings, showing a lower probability of having a child with autism after folic acid use37 during pregnancy, and more specifically, a child with autism and intellectual disability38. A meta-analysis of multiple studies showed this effect was not limited to one particular race or ethnicity39 and is present regardless of whether there was a strong genetic or environmental component to the diagnosis37,40. The recommendation to take folic acid prior to or during pregnancy is not unusual—it’s something that the March of Dimes has been telling women to do for decades to reduce birth defects. Also, gene/environment interactions, rather than the influence of one or the other, have again proven critical. Presence of a genetic mutation called a copy number variation, plus exposure to high levels of air pollution, showed an effect on diagnosis more than either by itself 41.
This year, the presence of gene/environment interactions was, for the first time, explored in terms of autism symptoms rather than probability of autism diagnosis. Rather than examine each genetic mutation individually, researchers examined environmental exposure with type of genetic mutation—either copy number variation or mutation—in likely autism genes. Two studies revealed that the combination, rather than each in isolation, increased autism severity scores in children with prenatal exposures and genetic factors42,43. This approach will open the doors to new ways to understand genetic and environmental contributions together, rather than in isolation, on different autism outcomes.
Some environmental factors have been shown to increase probability of a diagnosis in the absence of genetic susceptibilities. One such risk factor, maternal immune activation in response to an infection, has been shown to raise the probability of having a child with autism up to two-fold. This year, toxoplasmosis and herpes were added to the list of possible immune events that can increase risk44,45. More importantly, the mechanism by which maternal immune activation alters probability of diagnosis was better ascertained. While previous studies have hypothesized through animal models or epidemiological designs that circulating chemicals called cytokines, produced as a response to maternal immune activation, were the cause, newer findings in the cerebral spinal fluid in individuals with autism and autistic adults has not found this to be the case46. Rather, transcription of genes that control how the brain is connected and shaped during development can be altered with early immune activation47 and is thought to be more crucially involved. And it isn’t all forms of maternal immune activation, as the presence of fever specifically as part of the immune reaction is also an important component of the effect48.
Another environmental factor, spacing of pregnancies, was also replicated as a risk factor in a large study. Too little time or a large amount of time between pregnancies increased the risk of the second child having an autism diagnosis49. Better understanding of the mechanism by which this occurs could lead to factors that could preempt symptoms49.
Of importance to the community, some environmental factors have been dispelled as influencing a diagnosis. For example, new and advanced statistical techniques have unraveled the role of maternal depression from maternal antidepressant use, and found that the use of antidepressants itself was not sufficient to elevate the probability of having a child diagnosed with autism50. Also, rather than infertility treatments, infertility itself seems to be underlying the link between in vitro fertilization and autism51. Understanding of these relationships allows parents to have more informed conversations with their doctors about family planning.
Paternal and Grandparental Factors
Environmental exposures aren’t just a “mom thing,” either. Paternal exposures are also known to play a role. Both maternal and paternal prenatal exposures to asthma- causing agents have also been shown to be linked to autism52. Advanced paternal age, linked to autism in multiple studies previously, was also more carefully examined. The same researchers who studied the association to autism also quantified factors in older fathers that led to higher educational achievement in kids, and named them in aggregate as the “geek index53.” Those fathers with a higher “geek index” were more likely to have male children who went further in school and earned more money53. This outcome is clearly different from those with lower functioning autism, who may not be able to be independent. This shows that there are different pathways originating from the same place, which are associated with different outcomes. Paternal influence on outcome might possibly be explained through epigenetic mechanisms—the way environmental factors turn on and off genes during development. Exposures prior to pregnancy might affect both the sperm and egg of future generations, seen when there is a paternal effect. These changes in gene expression have been linked to a number of outcomes, including autism. They are not just observed in parental exposures, but in grand-parental exposures as well. These types of observations are incredibly hard to achieve, since outcomes need to be tracked across generations, through many decades. However, use of registry data or longitudinal studies where databases are linked on related individuals now makes this possible.
This year saw the first study of grand-parental exposure on later autism features. Grand-maternal smoking was linked to impaired scores on social communication measures and restrictive and repetitive behavior scales, which are independently predictive of an autism diagnosis54. Not only is it the first study to look beyond mother/father exposures, because this grandmaternal exposure affects the egg or sperm of subsequent generations, these findings advance the role of epigenetic mechanisms involved in autism. These include methylation, where methyl groups that are attached to areas of the DNA turn on and off gene expression, and histone acetylation, where DNA winds on histones, which may affect gene expression. Late last year, a project that investigated the cumulative effects of genetic mutations with environmental exposures was conducted in cell lines. This study showed new methylation marks on even more autism risk genes, which may cause genetic instability in areas of the genome outside the original mutation55. This opens up new ways to understand the role of genetic and environmental contributions to autism. However, because epigenetic marks are dependent on the tissue of interest, studying the brains of people with autism is essential to better understanding underlying causes of ASD.
It Takes Brains to Solve Autism
Credit: Ruth Weir, UC Davis MIND Institute
The Autism BrainNet provides brain tissue to researchers worldwide to not just discover the causes of autism, but also identify newer treatment targets, and pinpoint the underlying neurobiology of autism to better understand individuals with autism. The largest study to date on methylation in autism found greater levels of methylation in autism brains compared to those without autism, across the genome but also in particular patterns of DNA regions56. Looking more specifically at particular neurons in the cortex, areas that are more or less methylated in autism compared to those without autism were focused on the immune system and neurodevelopment57. Taken together, differential patterns of methylation in brain tissue may explain gene / environment interaction in autism.
But the autism discoveries, which are possible thanks to brain tissue, are not limited to causation. The region called the amygdala has been linked to autism through genetic, behavioral and structural neuroimaging studies. Looking at the cells in the amygdala, researchers find that the neuron length is longer and there are more sites of contact with other neurons on them in the autism brain58. However, these changes are age-dependent, as there are greater spine densities compared to controls in children and adolescents and less density compared to controls in adulthood, which may partially explain changes in symptoms of autism as people age58. Another clinically relevant finding is the loss of what are known as inhibitory neurons in the cortex of brains with autism. A decrease in signals that slow down neuronal activity in the brain may contribute to the dysregulation of too much or too little activity in multiple areas brain examined by different research groups59,60. In addition to a reduction in inhibitory neurons which help with the checks and balances of brain activity, there is evidence that cells that become neurons of the corpus callosum, the tract of fibers that connects the right and left hemisphere, do not develop properly 61. This is consistent with other studies using imaging techniques, which demonstrate that cells in the brain do not go to the right places or do not reach their final destinations accurately. These results also help explain some of the behavioral and biological signs of ASD.
The Big News This Year: Biology Before Behavior
Credit: Jason Wolff, University of Minnesota
Some of the most highly-publicized and possibly the most impactful findings from this year were multiple studies that looked at early biological signs, or biomarkers, of autism before autism symptoms emerge. One longitudinal research study, called the Infant Brain Imaging Study, tracked brain size and shape of infant siblings of those with an autism diagnosis, who have a 15x risk of being diagnosed themselves. In this way, biological features from as young as 6 months of age were tracked in infants to 2 years when autism diagnosis could be made. This allowed scientists the unprecedented ability to detect biological features prior to when even very early warning signs emerge, with the potential for even earlier detection and, hopefully, earlier intervention.
Earlier findings from the Infant Brain Imaging Study revealed that white fiber tracts grew at a slower rate in infants with autism compared to those who did not. While interesting, those findings were also preliminary. This year, a more detailed analysis of growth in infants with autism showed that increased surface area of the cortex from 6-12 months was tied to brain overgrowth at 12-18 months, which was then associated with social deficits62. The researchers then took this larger data set—MRIs of brain volume, surface area, cortical thickness at 6 and 12 months of age, and gender of the infants—and used a computer program to identify a way to classify babies most likely to meet criteria for autism at 24 months of age62. Now scientists are even closer to finding a biological method of detecting autism even before behavioral features emerge in babies with an older sibling with autism.
Credit: Mark Shen, University of North Carolina at Chapel Hill
This finding was followed by the discovery in the same dataset of the use of 6 months functional connectivity as an accurate predictor of autism diagnosis63 and identification of the circuit that controls a key feature of autism—joint attention64. Functional connectivity analyses at 6 months also revealed a different circuit for the emergence of repetitive behaviors and sensory sensitivities65. Later in the year, another analysis of the data revealed an 18% increase in cerebrospinal fluid outside the brain could be detected in those with autism as early as six months of age66.
While the Infant Brain Imaging Study was used to generate algorithms for earlier diagnosis, other investigations also revealed different interesting biological markers that need further study. For example, electroencephalographic (EEG, a measure of brain activity) markers in the frontal lobe of the brain were altered in three month-old infant siblings of those with autism, compared to those without an older sibling67. Another research group showed that, at seven months, EEG during a gaze shifting task improved the accuracy of a commonly used instrument to detect early signs and symptoms of autism in infants, the Autism Observational Scale in Infants68. This suggests that biological measures can enhance behavioral observation to predict ASD. At 18 months, compared to toddler siblings of those without an autism diagnosis, younger siblings of individuals with autism exhibited less synchronized activity between both sides of the brain. These infants showed higher levels of sensory seeking, which was linked to autism symptomatology69. This may open the door for earlier interventions focused on particular symptoms, reducing disability.
New Early Markers of Autism
Current larger scale studies are now examining the use of EEG as a biomarker for autism and how it is linked to symptoms. The convergence of data around neurological signs of autism, before even the time when symptoms are able to be detected by a trained clinician, shows the importance and power of infant siblings research design to identify the earliest biological signs. Earlier detection leads to expedition into early intervention. But it wasn’t just about biology. Another, even earlier, behavioral marker was revealed this year. This was to name which, when not present by nine months, predicts an earlier diagnosis of ASD and lower receptive language scores70. Pediatricians should be urged to consider this as an early warning sign of ASD.
The Autism Community Takes Part
The same biological markers used to aid in early detection of autism are also helping to understand how early interventions are affecting brain function. Following very early exposure to a parent-delivered intervention for those who have a 15x higher probability of an autism diagnosis (infant sibs), some of the brain activity markers changed within months after the intervention. This shows that parent-delivered interventions help to change both behaviors and brain function. And while parent-delivered interventions don’t necessarily lead to a change in autism diagnosis as a “yes or no” concept, longer term follow up of early infant interventions have, again, resulted in positive findings with regards to attentiveness and initiation of communication71, which may lead to even greater gains with longer follow-up, or higher level of functioning in those with a diagnosis. Of great importance to advocates making the case for getting these interventions covered by insurance, the cost savings realized in the long run in early interventions was documented through an economics approach72. Early intervention, not surprisingly, costs more in the beginning in terms of added services, but eventually more than makes up for those upfront costs through savings in fewer services needed in adolescence and adulthood72.
In the past, many intervention and treatment studies have met with difficulties because accurate measures to study change over time in people with autism have not been developed or validated. In order to address this challenge, new measures have been designed and tested. One uses biosensors to collect biological data including heart rate, eye tracking and a sleep monitor, which will be used in future clinical trials to incorporate biological markers into treatment outcome73. Another used a portal EEG machine to track brain activity during a variety of circumstances and settings74. Importantly, two new behavioral instruments incorporating parental feedback into the final product were validated this year. The first was the direct result of the Patient Centered Outcome Research Institute, funded by the Affordable Care Act. This measure asks parents to nominate their top concerns for later tracking of treatment response. This measure has been shown to be valid in tracking symptoms of ADHD in children with autism75. The other, the Autism Family Experience Questionnaire (AFEQ), was developed with consistent input of parent groups and consists of four domains relating to parental perspectives, child social functioning, family life and child symptoms76.
How Technologies Can Enhance Interventions
Credit: Tim Reckmann
Technology has also shown to be an important adjunct to intervention protocols. For example, the smartglass (previously known as Google Glass) has been repurposed by other companies and has been shown to be well tolerated and fun for both children and adults with autism77,78, reducing symptoms of ASD, such as challenging behaviors, and improving non-verbal communication77. Augmentative and alternative communication (AAC) devices have also been studied in a variety of settings over the past few years, but surprisingly, they have only been investigated for a limited range of communicative gestures, like requesting79,80. Now, they are being studied and proving helpful in conjunction with, rather than replacing, naturalistic behavioral interventions81. Further research should focus on using these devices for a wider range of communication skills.
iPads, which are used by so many families or individuals with autism, were not previously studied scientifically in terms of their use for different purposes. In a new study this year, however, a group examined if the iPad was really helpful in enhancing the effectiveness of a home-based parent-delivered intervention. In fact, use of the iPad led to short-term improvements in autism-related behaviors and an increase in certain skills; however, the amount of time kids used the iPad in conjunction with the intervention declined over time82. They were probably still using the device, but not for its intended use. Newer applications will need to provide additional ways to engage users for the purpose of intervention. Other therapies, such as music therapy, were shown in a randomized trial to be no better than other therapies for core autism symptoms83. However, if you or your family love music, don’t drop music therapy yet – there is no evidence to say it is harmful or doesn’t work as an adjunct to more proven intervention techniques. Many parents I know who use music therapy use it in conjunction with other techniques.
More Findings About Females, But Much More Is Needed
In 2015, this summary was titled “The Year of the Female” due to the increase in studies focused on females with autism. This year saw a continued explosion in the knowledge around females with autism and how sex differences in those without autism can help inform why females have different symptoms and different prevalence of ASD. In fact, an entire issue of the journal Autism was devoted to scientific investigations of females with ASD84. The topics of this issue ranged from impressions from clinicians and psychometrics of current assessment instruments in females to why the prevalence of autism is different in males compared to females. This last question has intrigued and frustrated researchers, because understanding this difference might lead to a better understanding of the causes, treatment and measurement of both males and females with ASD.
What Explains the Gender Gap?
While previously assumed to be 4:1, the M:F bias in autism might actually be less. A new review and meta-analysis of millions of people shows variability across studies and calls into questions the original 4:1 number85. However, even at 3:1, there is a considerable difference in prevalence in autism between males and females, and several theories about what’s behind this disparity.
One theory is that females, through better innate social communication abilities, are able to camouflage their symptoms and mask their diagnosis. This has been observed in the naturalistic setting of recess in elementary schools, illustrated by females showing compensatory behaviors in social situations86. Camouflaging was also operationalized by a research group who defined it as the difference between how someone feels on the inside (self-report measures of autism symptoms and measures of social cognition) compared to how they appear on the outside (observational measures)87. Using this methodology revealed higher camouflaging scores in females87, further reinforcing this as a potential mechanism for diagnostic disparity. Unfortunately, higher camouflage scores were also associated with higher markers of depression, indicating the need to recognize psychiatric issues in females with ASD.
Another hypothesis for the difference in prevalence is that females are protected against an autism diagnosis. This year, additional evidence was published that supports the concept of a female protective effect in autism. This protective effect may be seen in the siblings of autistic females. To examine this using the big data approach, the rate of autism diagnosis in families was examined when the first child was a male vs. the first child was a female. When the older sibling was a female, recurrence rate was 1.3x higher than if the older sibling was a male88. This is consistent with other data finding that autistic females have more genetic mutations that are also seen in family members, but don’t always translate to an ASD diagnosis—hence, a protective effect in females with this shared genetic burden.
The female protective effect was also observed with regards to prenatal androgen levels. In children whose older sibling was a male, there was no association between cord blood levels of androgen and either early autism scores or social responsiveness. However, if the older sibling was a female, there was a positive association between prenatal testosterone and autism at both 12 and 36 months89. This could mean that the shared genetic liability seen in siblings of females changes sensitivity to prenatal androgen exposure. Finally, the protective effect was observed in brain tissue of individuals with autism. Female brains showed more dysregulated RNA levels, particularly in immune system and nervous system pathways, demonstrating a greater genetic load in females despite a lower prevalence90, consistent with other studies examining the differences in gene expression in males and females with ASD.
Let’s Talk About Sex
Possibly due in part from pressure from the self-advocacy community for more and higher quality research to help and better understand adults with autism, more scientific findings were published relating to the specific challenges faced by adults with ASD.
First, most diagnostic tools have traditionally been geared towards children with ASD. A new instrument called the 3Di-Adult takes about 40 minutes to administer and was shown to be both sensitive and specific91 to diagnosing autism in adults, providing a resource for adults who previously had not received a formal diagnosis.
Studies focused on sexuality in people with autism almost tripled this year, and many of them reinforced what the Neuroqueer movement has been saying for a while: People with autism are less likely to affiliate with an established gender or sexual orientation92-95. Autistic females are more likely to have more sexual partners, but also more negative sexual experiences compared to males93. A new sexual education program was released that has shown to help with what might be the biggest issue in sexuality in autistic adolescents and adults: poor or incomplete sexual education96.
Autism and Employment Challenges
Another important issue affecting many autistic adults is employment. After 10 years of gathering data from vocational rehabilitation services, it appears that the only predictor of employment outcome is number, not type, of VR services, suggesting “the more the better97”. Outside VR services, other factors predicted successful sustained employment. These included better independent living skills, receiving an inclusive education, and living in an urban environment (probably due to transportation issues)98. The good news is that the research community is paying special attention to employment issues, supporting a policy brief for employment, and developing new types of programs.
Big Findings Come From Big Data
This was another exciting year for autism research, using big data to better understand and isolate the factors that make people with autism similar and different. Whether you are a person with autism, a family member, a service provider, or someone else affected by autism—regardless of whether you agree on the needs of people with autism, no matter the IQ or verbal ability of you or your child—progress is being made each year to make your life better.
While it may be difficult to see in the very short term, giant gains continue to be made thanks to scientific advances that can be seen after 5 years, or even a decade. It’s frustrating to be told to “just be patient,” but the “informed hope” we should all have is that science and research will continue to provide answers—answers that help everyone.
Thank You
The research and the progress in care thanks to scientific understanding of autism does not happen without families and individuals who give their time and effort for these studies. Thank you! Researchers also play an important role—it’s not an especially glamorous job and the hourly pay would be way below minimum wage. The contributions by the entire autism community make these things possible. Want to participate? Register for the Autism BrainNet at www.takesbrains.org. Answer a few questions and spit into a tube and you can become part of Spark at www.sparkforautism.org. Spark is exactly the sort of “big data” project that will help understanding of individuals across the spectrum and what makes them so different.
Pellicano E, Dinsmore A, Charman T. Views on researcher-community engagement in autism research in the United Kingdom: a mixed-methods study. PLoS One. 2014;9(10):e109946.
Pellicano E, Dinsmore A, Charman T. What should autism research focus upon? Community views and priorities from the United Kingdom. Autism. 2014;18(7):756-770.
Fletcher-Watson S, Larsen K, Salomone E, Members of the CEWG. What do parents of children with autism expect from participation in research? A community survey about early autism studies. Autism. 2017:1362361317728436.
Baron-Cohen S. Editorial Perspective: Neurodiversity – a revolutionary concept for autism and psychiatry. J Child Psychol Psychiatry. 2017;58(6):744-747.
Tiura M, Kim J, Detmers D, Baldi H. Predictors of longitudinal ABA treatment outcomes for children with autism: A growth curve analysis. Res Dev Disabil. 2017;70:185-197.
Solomon M, Iosif AM, Reinhardt VP, et al. What will my child’s future hold? phenotypes of intellectual development in 2-8-year-olds with autism spectrum disorder. Autism Res. 2017.
Kim SH, Bal VH, Lord C. Longitudinal follow-up of academic achievement in children with autism from age 2 to 18. J Child Psychol Psychiatry. 2017.
Visser JC, Rommelse NNJ, Lappenschaar M, Servatius-Oosterling IJ, Greven CU, Buitelaar JK. Variation in the Early Trajectories of Autism Symptoms Is Related to the Development of Language, Cognition, and Behavior Problems. J Am Acad Child Adolesc Psychiatry. 2017;56(8):659-668.
Barbaro J, Dissanayake C. Diagnostic stability of autism spectrum disorder in toddlers prospectively identified in a community-based setting: Behavioural characteristics and predictors of change over time. Autism. 2017;21(7):830-840.
Pathak M, Bennett A, Shui AM. Correlates of adaptive behavior profiles in a large cohort of children with autism: The autism speaks Autism Treatment Network registry data. Autism. 2017:1362361317733113.
Kraper CK, Kenworthy L, Popal H, Martin A, Wallace GL. The Gap Between Adaptive Behavior and Intelligence in Autism Persists into Young Adulthood and is Linked to Psychiatric Co-morbidities. J Autism Dev Disord. 2017;47(10):3007-3017.
Sparrow SS, Cicchetti, D.V., and Saulnier, C.A. . The Vineland Adaptive Behavior Scales, Third Edition. Bloomington, MN: NCS Pearson; 2016.
Wittke K, Mastergeorge AM, Ozonoff S, Rogers SJ, Naigles LR. Grammatical Language Impairment in Autism Spectrum Disorder: Exploring Language Phenotypes Beyond Standardized Testing. Front Psychol. 2017;8:532.
Wiggins LD, Tian LH, Levy SE, et al. Homogeneous Subgroups of Young Children with Autism Improve Phenotypic Characterization in the Study to Explore Early Development. J Autism Dev Disord. 2017;47(11):3634-3645.
Mazurek MO, Lu F, Symecko H, et al. A Prospective Study of the Concordance of DSM-IV and DSM-5 Diagnostic Criteria for Autism Spectrum Disorder. J Autism Dev Disord. 2017.
Grzadzinski R, Lord C, Sanders SJ, Werling D, Bal VH. Children with autism spectrum disorder who improve with fever: Insights from the Simons Simplex Collection. Autism Res. 2017.
Weiner DJ, Wigdor EM, Ripke S, et al. Polygenic transmission disequilibrium confirms that common and rare variation act additively to create risk for autism spectrum disorders. Nat Genet. 2017;49(7):978-985.
Turner TN, Coe BP, Dickel DE, et al. Genomic Patterns of De Novo Mutation in Simplex Autism. Cell. 2017;171(3):710-722 e712.
Bishop SL, Farmer C, Bal V, et al. Identification of Developmental and Behavioral Markers Associated With Genetic Abnormalities in Autism Spectrum Disorder. Am J Psychiatry. 2017;174(6):576-585.
Hudac CM, Stessman HAF, DesChamps TD, et al. Exploring the heterogeneity of neural social indices for genetically distinct etiologies of autism. J Neurodev Disord. 2017;9:24.
Arnett AB, Cairney BE, Wallace AS, et al. Comorbid symptoms of inattention, autism, and executive cognition in youth with putative genetic risk. J Child Psychol Psychiatry. 2017.
Tylee DS, Hess JL, Quinn TP, et al. Blood transcriptomic comparison of individuals with and without autism spectrum disorder: A combined-samples mega-analysis. Am J Med Genet B Neuropsychiatr Genet. 2017;174(3):181-201.
van Rooij D, Anagnostou E, Arango C, et al. Cortical and Subcortical Brain Morphometry Differences Between Patients With Autism Spectrum Disorder and Healthy Individuals Across the Lifespan: Results From the ENIGMA ASD Working Group. Am J Psychiatry. 2017:appiajp201717010100.
RK CY, Merico D, Bookman M, et al. Whole genome sequencing resource identifies 18 new candidate genes for autism spectrum disorder. Nat Neurosci. 2017;20(4):602-611.
Lim ET, Uddin M, De Rubeis S, et al. Rates, distribution and implications of postzygotic mosaic mutations in autism spectrum disorder. Nat Neurosci. 2017;20(9):1217-1224.
Krupp DR, Barnard RA, Duffourd Y, et al. Exonic Mosaic Mutations Contribute Risk for Autism Spectrum Disorder. Am J Hum Genet. 2017;101(3):369-390.
Constantino JN, Kennon-McGill S, Weichselbaum C, et al. Infant viewing of social scenes is under genetic control and is atypical in autism. Nature. 2017;547(7663):340-344.
Autism Spectrum Disorders Working Group of The Psychiatric Genomics C. Meta-analysis of GWAS of over 16,000 individuals with autism spectrum disorder highlights a novel locus at 10q24.32 and a significant overlap with schizophrenia. Mol Autism. 2017;8:21.
St Pourcain B, Eaves LJ, Ring SM, et al. Developmental Changes Within the Genetic Architecture of Social Communication Behavior: A Multivariate Study of Genetic Variance in Unrelated Individuals. Biol Psychiatry. 2017.
Ben-Shalom R, Keeshen CM, Berrios KN, An JY, Sanders SJ, Bender KJ. Opposing Effects on NaV1.2 Function Underlie Differences Between SCN2A Variants Observed in Individuals With Autism Spectrum Disorder or Infantile Seizures. Biol Psychiatry. 2017;82(3):224-232.
Escamilla CO, Filonova I, Walker AK, et al. Kctd13 deletion reduces synaptic transmission via increased RhoA. Nature. 2017;551(7679):227-231.
Stoodley CJ, D’Mello AM, Ellegood J, et al. Altered cerebellar connectivity in autism and cerebellar-mediated rescue of autism-related behaviors in mice. Nature Neuroscience. 2017;20(12):1744-1751.
Raghavan R, Riley AW, Volk H, et al. Maternal Multivitamin Intake, Plasma Folate and Vitamin B12 Levels and Autism Spectrum Disorder Risk in Offspring. Paediatr Perinat Epidemiol. 2017.
DeVilbiss EA, Magnusson C, Gardner RM, et al. Antenatal nutritional supplementation and autism spectrum disorders in the Stockholm youth cohort: population based cohort study. BMJ. 2017;359:j4273.
Wang M, Li K, Zhao D, Li L. The association between maternal use of folic acid supplements during pregnancy and risk of autism spectrum disorders in children: a meta-analysis. Mol Autism. 2017;8:51.
Goodrich AJ, Volk HE, Tancredi DJ, et al. Joint effects of prenatal air pollutant exposure and maternal folic acid supplementation on risk of autism spectrum disorder. Autism Res. 2017.
Kim D, Volk H, Girirajan S, et al. The joint effect of air pollution exposure and copy number variation on risk for autism. Autism Res. 2017;10(9):1470-1480.
Webb SJ, Garrison MM, Bernier R, McClintic AM, King BH, Mourad PD. Severity of ASD symptoms and their correlation with the presence of copy number variations and exposure to first trimester ultrasound. Autism Res. 2017;10(3):472-484.
Ackerman S, Schoenbrun S, Hudac C, Bernier R. Interactive Effects of Prenatal Antidepressant Exposure and Likely Gene Disrupting Mutations on the Severity of Autism Spectrum Disorder. J Autism Dev Disord. 2017;47(11):3489-3496.
Spann MN, Sourander A, Surcel HM, Hinkka-Yli-Salomaki S, Brown AS. Prenatal toxoplasmosis antibody and childhood autism. Autism Res. 2017;10(5):769-777.
Mahic M, Mjaaland S, Bovelstad HM, et al. Maternal Immunoreactivity to Herpes Simplex Virus 2 and Risk of Autism Spectrum Disorder in Male Offspring. mSphere. 2017;2(1).
Pardo CA, Farmer CA, Thurm A, et al. Serum and cerebrospinal fluid immune mediators in children with autistic disorder: a longitudinal study. Mol Autism. 2017;8:1.
Lombardo MV, Moon HM, Su J, Palmer TD, Courchesne E, Pramparo T. Maternal immune activation dysregulation of the fetal brain transcriptome and relevance to the pathophysiology of autism spectrum disorder. Mol Psychiatry. 2017.
Hornig M, Bresnahan MA, Che X, et al. Prenatal fever and autism risk. Mol Psychiatry. 2017.
Schieve LA, Tian LH, Drews-Botsch C, et al. Autism spectrum disorder and birth spacing: Findings from the study to explore early development (SEED). Autism Res. 2017.
Oberlander TF, Zwaigenbaum L. Disentangling Maternal Depression and Antidepressant Use During Pregnancy as Risks for Autism in Children. JAMA. 2017;317(15):1533-1534.
Schieve LA, Drews-Botsch C, Harris S, et al. Maternal and Paternal Infertility Disorders and Treatments and Autism Spectrum Disorder: Findings from the Study to Explore Early Development. J Autism Dev Disord. 2017;47(12):3994-4005.
Singer AB, Burstyn I, Thygesen M, Mortensen PB, Fallin MD, Schendel DE. Parental exposures to occupational asthmagens and risk of autism spectrum disorder in a Danish population-based case-control study. Environ Health. 2017;16(1):31.
Janecka M, Rijsdijk F, Rai D, Modabbernia A, Reichenberg A. Advantageous developmental outcomes of advancing paternal age. Transl Psychiatry. 2017;7(6):e1156.
Golding J, Ellis G, Gregory S, et al. Grand-maternal smoking in pregnancy and grandchild’s autistic traits and diagnosed autism. Sci Rep. 2017;7:46179.
Dunaway KW, Islam MS, Coulson RL, et al. Cumulative Impact of Polychlorinated Biphenyl and Large Chromosomal Duplications on DNA Methylation, Chromatin, and Expression of Autism Candidate Genes. Cell Rep. 2016;17(11):3035-3048.
Ellis SE, Gupta S, Moes A, West AB, Arking DE. Exaggerated CpH methylation in the autism-affected brain. Mol Autism. 2017;8:6.
Nardone S, Sams DS, Zito A, Reuveni E, Elliott E. Dysregulation of Cortical Neuron DNA Methylation Profile in Autism Spectrum Disorder. Cereb Cortex. 2017;27(12):5739-5754.
Weir RK, Bauman MD, Jacobs B, Schumann CM. Protracted dendritic growth in the typically developing human amygdala and increased spine density in young ASD brains. J Comp Neurol. 2017.
Hashemi E, Ariza J, Rogers H, Noctor SC, Martinez-Cerdeno V. The Number of Parvalbumin-Expressing Interneurons Is Decreased in the Prefrontal Cortex in Autism. Cereb Cortex. 2017:1.
Adorjan I, Ahmed B, Feher V, et al. Calretinin interneuron density in the caudate nucleus is lower in autism spectrum disorder. Brain. 2017;140(7):2028-2040.
Wegiel J, Flory M, Kaczmarski W, et al. Partial Agenesis and Hypoplasia of the Corpus Callosum in Idiopathic Autism. J Neuropathol Exp Neurol. 2017;76(3):225-237.
Hazlett HC, Gu H, Munsell BC, et al. Early brain development in infants at high risk for autism spectrum disorder. Nature. 2017;542(7641):348-351.
Emerson RW, Adams C, Nishino T, et al. Functional neuroimaging of high-risk 6-month-old infants predicts a diagnosis of autism at 24 months of age. Sci Transl Med. 2017;9(393).
Eggebrecht AT, Elison JT, Feczko E, et al. Joint Attention and Brain Functional Connectivity in Infants and Toddlers. Cereb Cortex. 2017;27(3):1709-1720.
Wolff JJ, Swanson MR, Elison JT, et al. Neural circuitry at age 6 months associated with later repetitive behavior and sensory responsiveness in autism. Mol Autism. 2017;8:8.
Shen MD, Kim SH, McKinstry RC, et al. Increased Extra-axial Cerebrospinal Fluid in High-Risk Infants Who Later Develop Autism. Biol Psychiatry. 2017;82(3):186-193.
Levin AR, Varcin KJ, O’Leary HM, Tager-Flusberg H, Nelson CA. EEG power at 3 months in infants at high familial risk for autism. J Neurodev Disord. 2017;9(1):34.
Bedford R, Gliga T, Shephard E, et al. Neurocognitive and observational markers: prediction of autism spectrum disorder from infancy to mid-childhood. Mol Autism. 2017;8:49.
Damiano-Goodwin CR, Woynaroski TG, Simon DM, et al. Developmental sequelae and neurophysiologic substrates of sensory seeking in infant siblings of children with autism spectrum disorder. Dev Cogn Neurosci. 2017.
Miller M, Iosif AM, Hill M, Young GS, Schwichtenberg AJ, Ozonoff S. Response to Name in Infants Developing Autism Spectrum Disorder: A Prospective Study. J Pediatr. 2017;183:141-146 e141.
Green J, Pickles A, Pasco G, et al. Randomised trial of a parent-mediated intervention for infants at high risk for autism: longitudinal outcomes to age 3 years. J Child Psychol Psychiatry. 2017;58(12):1330-1340.
Cidav Z, Munson J, Estes A, Dawson G, Rogers S, Mandell D. Cost Offset Associated With Early Start Denver Model for Children With Autism. J Am Acad Child Adolesc Psychiatry. 2017;56(9):777-783.
Ness SL, Manyakov NV, Bangerter A, et al. JAKE(R) Multimodal Data Capture System: Insights from an Observational Study of Autism Spectrum Disorder. Front Neurosci. 2017;11:517.
Billeci L, Tonacci A, Tartarisco G, et al. An Integrated Approach for the Monitoring of Brain and Autonomic Response of Children with Autism Spectrum Disorders during Treatment by Wearable Technologies. Front Neurosci. 2016;10:276.
Scahill L, Bearss K, Sarhangian R, et al. Using a Patient-Centered Outcome Measure to Test Methylphenidate Versus Placebo in Children with Autism Spectrum Disorder. J Child Adolesc Psychopharmacol. 2017;27(2):125-131.
Leadbitter K, Aldred C, McConachie H, et al. The Autism Family Experience Questionnaire (AFEQ): An Ecologically-Valid, Parent-Nominated Measure of Family Experience, Quality of Life and Prioritised Outcomes for Early Intervention. J Autism Dev Disord. 2017.
Liu R, Salisbury JP, Vahabzadeh A, Sahin NT. Feasibility of an Autism-Focused Augmented Reality Smartglasses System for Social Communication and Behavioral Coaching. Front Pediatr. 2017;5:145.
Keshav NU, Salisbury JP, Vahabzadeh A, Sahin NT. Social Communication Coaching Smartglasses: Well Tolerated in a Diverse Sample of Children and Adults With Autism. JMIR Mhealth Uhealth. 2017;5(9):e140.
Holyfield C, Drager KDR, Kremkow JMD, Light J. Systematic review of AAC intervention research for adolescents and adults with autism spectrum disorder. Augment Altern Commun. 2017;33(4):201-212.
Logan K, Iacono T, Trembath D. A systematic review of research into aided AAC to increase social-communication functions in children with autism spectrum disorder. Augment Altern Commun. 2017;33(1):51-64.
Chang YC, Shih W, Landa R, Kaiser A, Kasari C. Symbolic Play in School-Aged Minimally Verbal Children with Autism Spectrum Disorder. J Autism Dev Disord. 2017.
Whitehouse AJO, Granich J, Alvares G, et al. A randomised controlled trial of an iPad-based application to complement early behavioural intervention in Autism Spectrum Disorder. J Child Psychol Psychiatry. 2017;58(9):1042-1052.
Crawford MJ, Gold C, Odell-Miller H, et al. International multicentre randomised controlled trial of improvisational music therapy for children with autism spectrum disorder: TIME-A study. Health Technol Assess. 2017;21(59):1-40.
Mandy W, Lai MC. Towards sex- and gender-informed autism research. Autism. 2017;21(6):643-645.
Loomes R, Hull L, Mandy WPL. What Is the Male-to-Female Ratio in Autism Spectrum Disorder? A Systematic Review and Meta-Analysis. J Am Acad Child Adolesc Psychiatry. 2017;56(6):466-474.
Dean M, Harwood R, Kasari C. The art of camouflage: Gender differences in the social behaviors of girls and boys with autism spectrum disorder. Autism. 2017;21(6):678-689.
Lai MC, Lombardo MV, Ruigrok AN, et al. Quantifying and exploring camouflaging in men and women with autism. Autism. 2017;21(6):690-702.
Palmer N, Beam A, Agniel D, et al. Association of Sex With Recurrence of Autism Spectrum Disorder Among Siblings. JAMA Pediatr. 2017;171(11):1107-1112.
Park BY, Lee BK, Burstyn I, et al. Umbilical cord blood androgen levels and ASD-related phenotypes at 12 and 36 months in an enriched risk cohort study. Mol Autism. 2017;8:3.
Schumann CM, Sharp FR, Ander BP, Stamova B. Possible sexually dimorphic role of miRNA and other sncRNA in ASD brain. Mol Autism. 2017;8:4.
Mandy W, Clarke K, McKenner M, et al. Assessing Autism in Adults: An Evaluation of the Developmental, Dimensional and Diagnostic Interview-Adult Version (3Di-Adult). J Autism Dev Disord. 2017.
George R, Stokes MA. Sexual Orientation in Autism Spectrum Disorder. Autism Res. 2017.
Hancock GIP, Stokes MA, Mesibov GB. Socio-sexual functioning in autism spectrum disorder: A systematic review and meta-analyses of existing literature. Autism Res. 2017;10(11):1823-1833.
Turner D, Briken P, Schottle D. Autism-spectrum disorders in adolescence and adulthood: focus on sexuality. Curr Opin Psychiatry. 2017;30(6):409-416.
May T, Pang KC, Williams K. Brief Report: Sexual Attraction and Relationships in Adolescents with Autism. J Autism Dev Disord. 2017;47(6):1910-1916.
Dekker LP, van der Vegt EJM, van der Ende J, et al. Psychosexual Functioning of Cognitively-able Adolescents with Autism Spectrum Disorder Compared to Typically Developing Peers: The Development and Testing of the Teen Transition Inventory- a Self- and Parent Report Questionnaire on Psychosexual Functioning. J Autism Dev Disord. 2017;47(6):1716-1738.
Alverson CY, Yamamoto SH. VR Employment Outcomes of Individuals with Autism Spectrum Disorders: A Decade in the Making. J Autism Dev Disord. 2017.
Chan W, Smith LE, Hong J, Greenberg JS, Lounds Taylor J, Mailick MR. Factors associated with sustained community employment among adults with autism and co-occurring intellectual disability. Autism. 2017:1362361317703760.
A 2018 Year End Review of Scientific Research
By Alycia Halladay, PhD, Chief Science Officer of the Autism Science Foundation and the Scientific Advisory Board of the Autism Science Foundation
Researchers have known for some time that individuals with autism spectrum disorder (ASD) and their family members show increased rates of psychiatric conditions including anxiety, depression, and attention deficit hyperactivity disorder (ADHD). A staggering one third of children with ASD also have those one or more of those disorders.1 This year’s research has given the community a deeper understanding of the biological connections between these conditions, shared genetics, and why ASD may be part of a larger spectrum of psychiatric issues affecting children and adults.
Crossover in diagnosis and in genetic profiles
Until the recent changes in the Diagnostic and Statistical Manual(DSM) (a psychiatric handbook used by doctors, therapists, and others in the U.S. to diagnose mental, behavioral, and developmental disorders), 1a person could not receive a diagnosis of both ASD and ADHD, so the clinician normally chose one or the other. Researchers only focused on the presence of ADHD orASD in families, rather than the crossover. Recently, researchers looked at first-degree relatives (parents, siblings, and children) and found a higher rate of ASD among those with ADHD and ASD2 as well as bipolar disorder3and schizophrenia4. A recent study that looked at all of the previous studies of anxiety that occurred alongside of ASD showed that adults with ASD were twenty times more likely to have anxiety and much more likely to have obsessive compulsive disorder (OCD) than people without ASD7. Evidence from young children suggest that there is great overlap in early predictors of anxiety and autism, which may diverge as children get older, forming two separate disorders8. By focusing in on those with co-occurring diagnoses or enriched family history, scientists see distinct cognitive profiles 5and behavioral features6. This means that while there is crossover, there may also be specific subgroups of ASD formed by the presence of co-occuring psychiatric symptoms.
Another study showed that co-occurring psychiatric disorders like depression and anxiety may be related to the gastrointestinal issues experienced in people with ASD9. This research provides further evidence that people with autism and their family members need thorough evaluations for mental health issues. Unfortunately, people with autism have a higher rate of unmet mental health needs than other groups10. The results of this study along with follow-up research published this year, identify factors such as availability of family centered care11and out of pocket co-pays12which affect access to the help that families need.
Anecdotally, the Autism Science Foundation often hears from family members of those with ASD wondering if a family history of a multitude of psychiatric issues had anything to do with the ASD diagnosis. The answer now is probably closer to a ‘yes’ than it was before, but that does not mean that anybody should ever feel guilty about another person’s diagnosis.
Based on these numbers, it is not surprising that several psychiatric issues, including ASD, all share common underlying genetic mechanisms. First, looking at the genetic profile of brain tissue obtained from the cortex of individuals affected by ASD, schizophrenia, bipolar depression and major depressive disorder, scientists revealed overlap in genetic expression. This overlap was highest between ASD, schizophrenia and bipolar depression13. While there is overlapping genetics, the brains of people with schizophrenia have a distinct lipid profile compared to autism, suggesting that schizophrenia, unlike autism, looks like accelerated aging in the brain.14Also, critical research from brains of people with autism compared to schizophrenia and bipolar disorder show that while gene are expressed similarly, the tiniest differences lead to different outcomes. Those with schizophrenia and bipolar depression express different isoforms, or end products of gene expression, which markedly changes what proteins are made15. These proteins are then what differentiate autism from schizophrenia.
Turning to analyses of gene function across these overlapping genes, these three disorders also showed similar impact of synaptic genes and those affecting the central nervous immune system13. Another landmark study included genetic information over 1 million people worldwide, including those with 17 different psychiatric (such as autism) and neurological (like Parkinson’s Disease) disorders. Psychiatric disorders were more similar to each other in genetic profiles than they were to neurological disorders, and while autism showed distinct genetic features, it overlapped with schizophrenia16. The sample used included mostly those with high intellectual ability and college attainment, so it is possible that some other relationships were not observed because of the heterogeneity of symptoms. Also of interest, ASD, ADHD, and schizophrenia are psychiatric issues with high genetic influence with similar trends in calculation of heritability across these three disorders 17. The differences across studies in heritability estimates are likely the result of all three of these conditions being the result of a variety of genetic and environmental factors, and differences in genetic factors within each disorder. No one gene causes schizophrenia, bipolar depression and autism, and even though there is overlap, it is unlikely that the same gene causes all three. While ASD can be considered an umbrella, it is now more likely than ever that schizophrenia, ADHD, and bipolar disorder are a larger umbrella over the autism umbrella. Scientists note that misdiagnosis occurs frequently between these disorders, so some genetic overlap is probably not surprising.
Exploiting genetic differences for new treatments
Given these findings, it seems important to include these other disorders when researching autism to identify commonalities and differences to exploit any therapeutic successes one disorder has had. That does not mean that what works in one group is always going to work in another group, but it can begin an important scientific conversation. Differences within the autism spectrum are seen in syndromes with a high prevalence of autism. For example, people with Phelan-McDermid Syndrome, or PMS, have autism about 70% of the time18. About 75% of people with Fragile X syndrome also have ASD19. Given this overlap, researchers have started to find out which interventions work for forms of ASD with and without known causes 20-21. Because people with a syndromic form of autism are more similar to each other than those without an established genetic link, starting from a place where there are fewer behavioral differences will provide answers, maybe even faster, than if scientists only studied those with no known established genetic link.
A new collaboration across these different rare genetic groups, called AGENDA, was formed this year. AGENDA will allow patient advocacy groups to share solutions to common problems experienced in research and by families.
One example of scientific evidence why these different rare genetic disorders overlap comes from brain tissue research. Researchers who study the brains of people with autism examined a protein, called FMRP, which is missing in people with Fragile X syndrome. They looked for this protein in those with a genetic form of autism called Dup15q Syndrome, as well as those with idiopathic autism. Idiopathic autism is a term for those with no known genetic cause of autism. The researchers found similarities between expression of FMRP in the same brain areas of those with autism and a known genetic mutation of chromosome 15 (Dup15q Syndrome), as well as idiopathic autism22. This could mean that targeting FMRP is a viable therapeutic option for all forms of ASD, regardless of genetic makeup. These findings would not be possible without the Autism BrainNet, a resource that supports the collection and analysis of brains of people with autism.
To learn more about the Autism BrainNet, and importantly, to register to receive information every quarter on the progress of research thanks to studying brain tissue, go to www.takesbrains.org/signup.
New prevalence estimates, old numbers
The question of “how many people have an autism diagnosis” seems to have a different answer depending on when, where, and how you ask. This year was no different. Global prevalence numbers across the world continue to be collected and analyzed and are influenced by culture, stigma, and the availability of diagnostic measures. Within the U.S., epidemiologists again saw two different prevalence numbers. The first, 1:59, was collected using the Autism and Developmental Disabilities Monitoring Network, examining educational records of those who had received a formal diagnosis24. It matches prevalence numbers from 2016. The other number came from an online or mail survey, previously a telephone survey, which asked parents whether they had a child with an ASD diagnosis. That number was reported in November 2018 as 1:4010. Different scientists have argued the advantages and disadvantages of each methodology, and they both have their strengths and weaknesses.
A prevalence study of autism diagnosis across time from Denmark might help reconcile this difference in numbers. As it turns out, prevalence of ASD rose in Denmark with age, as there are additional opportunities through school age to be identified25. In that study, the prevalence of ASD was the highest reported so far: 1:35 in 16 year olds born in 2000-2001, suggesting for the first time that prevalence may change with age. Since the ADDM study examined 8 year olds, and the 1:40 study examined children across different ranges, age may be a factor in prevalence. Additional data from the U.S. suggests that a small group of individuals who miss the diagnostic cutoff at age three, might meet it at age five26. There are some kids who teeter on a diagnosis for years. Whether or not 1:59 or 1:40 is closer to the true prevalence of autism still remains to be seen, but the MMWR does report unique: it further illustrates the racial and ethnic disparity in access to diagnosis seen in the U.S.24 More work in better identifying people with autism at different ages, and from different backgrounds, so nobody is missed, is sorely needed.
Where are the girls?
There is also a disparity in diagnosis between males and females, and while exact ratio of 4:1 males to females diagnosed has been questioned, there is a real and consistent difference in the number of men vs. women diagnosed with ASD. Researchers are searching for the causes of these differences, and how they change over time. For example, young females with autism show better attention to social scenes, which may reduce autism severity and lead to fewer diagnoses in girls27. In addition, as children, the special and restricted interests of girls are different from boys’ interests. That is, there preferences are similar to neurotypical girls 28. These differences may potentially lead to some girls with autism being missed. In a subset of females with autism, specifically those that have higher intellectual abilities, some show more typical brain responses compared to males29, suggesting they can mask their symptoms.
However, researchers cannot rule out a biological underpinning of a sex bias. Sex hormones (androgens) at critical areas of development can influence the function of brain circuits associated with autism, and a sex bias as a result of hormone exposure or alteration in hormone levels is possible30. During key points in brain cell development, these hormones can cause the cells to divide too quickly and affects disruptions in how cells turn into brain cells or other types of cells in the body31, which are features of cells in autism. Unfortunately, many studies looking at environmental factors that lead to autism in males and female children have either not shown a difference across sex, or not looked at sex of the child 32-34. This prevents researchers from determining whether these environmental factors result in a sex bias. The presence of the core features of autism seem to be similar for both males and females, though they may differ by severity or age. For example, in a large study conducted in the U.K., males started out with higher autistic social traits, but as adolescence approached, that was no longer the case35. Features of autism in males and females, may change over time, or get more or less severe, depending on sex.
If the core symptoms are present in females, why are fewer females diagnosed? This continues to be an important area of research. We do know that females do not escape the conditions that occur alongside ASD. Previous research has shown a higher level of internalizing behavior in females with ASD. Internalizing behaviors are those that are inwardly expressed, including depression and anxiety. Externalizing, or outwardly expressed behaviors, include acting-out behaviors such as aggression or impulsivity. This year, scientists examined another outward symptom: hoarding. Children with autism are five times more likely to show hoarding behavior . This is similar to the hoarding rates in ADHD and OCD36, with girls showing more hoarding behavior than boys do.
Genes and environment, not genes or the environment
Since environmental factors were just mentioned with regards to sex differences, it should be noted that while environmental factors may not account for the sex bias in autism, they continue to be investigated and reported as influence in an ASD diagnosis. For example, there continues to be mounting evidence that air toxins, including air pollution, produces an increased probability of having a child with autism33,34,37. Since the type and source of air pollution varies by country and region, it is not surprising that there may be some variability in the findings – with some studies showing an effect of one chemical, and others another component of air pollution. Air pollution as a whole should be of high concern across the world, and research should continue to build scientific evidence of its harmful effects, not just in autism, but also in many developmental disorders. A chemical which scientists thought was no longer a problem because it had been banned 20 years ago, was recently associated with autism38. While the effect was not large, it should serve as a reminder that known toxicants don’t always disappear when legislation changes, or manufacturing processes evolve. Other maternal health factors have been shown to influence later autism diagnosis, from polycystic ovarian syndrome in mother32, history of immune issues39, and even opioid use before conception40.
Though it is important to find factors that may contribute to autism, it is also very important to identify factors that don’t contribute to autism. This year, researchers in Scandinavia were able to dispel the theory that autism is caused by too many antibiotics given because of frequent ear infections41.
While scientists continue to make significant progress in understanding the role of genetics and genetic influence in autism risk, they were unable to better illustrate the mechanisms by which genes and the environment interact. However, new ways to study the environment in autism have emerged. Researchers were able to show the feasibility of using baby teeth to study environmental exposures during pregnancy. Because the layers of the teeth form like rings on a tree during gestation, each layer can be analyzed precisely to examine month-to-month environmental exposure or change in metabolism. This year, researchers who examined baby teeth of those with a later autism diagnosis, found that the normal cycles of zinc and copper, which occur as part of normal biological processes, were altered in ASD42. This might reflect an inability to detoxify the body following an exposure during pregnancy. However, that theory needs further study.
Also in 2018, researchers used brain tissue to show that genes relating to mitochondrial function were altered in those with autism, and the changes correlated to genes which affect how brain cells, or neurons, are shaped and function. These findings suggest that mitochondria, which are the targets of environmental factors, may act by altering the function of autism-related genes43.
In the past decade, researchers have added greatly to the understanding of autism genetics. And many of these discoveries are actionable by families! Because whole genome sequencing technologies have become more accessible and available to more research labs, new types of genetic contributions are being discovered. In the past, geneticists have focused on areas of the genome which code for proteins, as these are the areas there were thought to have the most influential effect on brain development. In late 2018, thanks to newer genetic technologies, new parts of the genome were able to be studied in relation to autism. They include regions of the DNA which serve as traffic lights – either stopping or starting the reading of genes from the genome44. They are called “promotor regions”. I’ll mention other areas of the DNA that were discovered to be associated with autism a little later. Past research has demonstrated that these more detailed genetic analyses can identify mutations that are targets of pharmacological therapy, and new emphasis on variations in the genome outside the traditional areas can lead to newer therapies.
It is likely that there will be an increase in the discovery of rare genetic mutations that strongly influence autism diagnosis. One type of mutation, called de novo mutations, are not seen in either parent, but are seen in the diagnosed individual. These gene changes sometimes overlap with autism, intellectual disability, and those that are involved in brain function. Right now, there are about two dozen rare de novo gene mutations accounting for about 10% of the cases of autism. With more information from whole genome sequencing, this percent may increase.
But what about the rest of autism? Is it all caused by de novo mutations that occur spontaneously? There is another type of mutation called common variation. The theory behind common variation is that autism symptoms are a spectrum, and to some degree everyone may fall on some part of the spectrum of autism traits. These traits may correspond to specific genetic signals. In most cases, autism develops from the right combination of , or too many, common variants, including known autism risk genes and those that aren’t associated with autism. This year, the percent of individuals with autism with common variants was estimated at around 8%94. As mentioned earlier, scientists now believe autism sits on the spectrum with other psychological issues and therefore, the genes associated with traits in the parents can combine, leading to increased chances that the child will receive an autism diagnosis45. Some of these are inherited, some may be de-novo, but they are not always inherited as autism genes, they can be inherited as common variations across the genome. More evidence comes from understanding the broader autism phenotype in families. Instead of looking at individuals with autism and their siblings, researchers explored genetic markers in all family members like parents, including ones with the broader autism phenotype, and found overlap in some of the genetic markers46. Even within families with lots of differences in clinical presentation of symptoms, there are some overlapping genetic factors. This demonstrates the importance of common variation in autism. However, it’s important to distinguish common variation that determines the color of our skin, to common variation which leads to autism. Common variation does not mean that genes associated with hair color can combine and lead to autism. These genes involved in common variation are known to control the way different brain regions connect with each other, how brain cells are shaped, and how they function. Common variation means that there may be different subgroups of autism caused by different subgroups of genes that can be inherited and de novo. And this expands what scientists learned last year, that common variation works together with rare variation, it’s not one or the other.
Mutations in promotor regions seen in people with ASD. From An et al., 2018.
Now back to new genetic findings thanks to whole genome sequencing. As explained earlier, new areas of the genome are able to be studied thanks to new genetic technologies. Two different research groups discovered this year that other areas, called non-coding regions, harbor variants that confer risk for autism47,48. Those promotor regions discussed earlier are also non-coding regions, but these studies looked at expression in family members. Using this design, geneticists calculated that the origin, while not the mutation but the origin of the mutation, came from the father’s side47and a model of combined influence of paternal and maternal factors to generate these seemingly “new” or “de novo” mutations emerged 47,48. It should be noted, however, that these findings should be viewed with caution because there are a lot of different places to look on the entire genome and scientists may need to adjust their statistical analysis techniques to make sure their findings are not by chance49. In other words, stay tuned. What geneticists continue to be excited about is the discovery of new genes that are targets of existing therapeutics and can explain co-occuring medical or psychiatric symptoms45. A better understanding of these targets is needed, which is why animal models are so important.
Animals don’t have autism, but they can tell scientists a lot about autism
Photo courtesy of Jill Silverman, UC Davis
Once scientists identify a target in the brain of someone with autism, it might take years of effort, money, and patience for that discovery to turn into something that can help people. This is a difficult wait, but it can pay off. This year, a new drug received fast track approval to treat the core symptoms of autism: balovaptan50. It targets the vasopressin receptor. It has been shown to positively influence social interaction and social communication in adults. But the road to balovaptan had to start with animal models – not just to see if it works but also to explore what dose, and what behaviors were the most promising to target in people.
These models are becoming more sophisticated, more specific, and with each model comes a better approximation of autism symptoms. For example, researchers are using rats to examine social communication deficits that better approximate conversation51. To be clear, autism is specifically human, but new therapies are becoming closer to real possibilities with the help of these models– for what works, and what does not. For example, environmental enrichment (a rough approximation of behavioral intervention in rodents) has been shown to be beneficial in some models of autism, but not so in genetic models like SHANK3 knockouts52. Parents of those whose children did not benefit from behavioral intervention see this as a possible explanation for why they haven’t seen progress. However, it does not mean that early behavioral intervention is not effective but that behavioral intervention may not work as well as in others for a variety of reasons, including genetics. These models have identified existing drugs can target autism-related behaviors in SHANK models of ASD53. These animal models can also help researchers identify similarities and differences on a cellular level between neurodevelopmental disorders, including ADHD and ASD54, narrow down the mechanism of sex differences in autism,55as well as better understand the contribution of individual genes to ASD as part of a larger group of genetic mutations, which is the case with most people with ASD56.
Another important model for autism is the use of cells
Example of groups of stem cells in a dish, called “organoids”
obtained from people with ASD. Researchers are able to turn skin cells into embryonic-like cells, called induced pluripotent stem cells, and then into brain cells, or any type of cell they want. Isn’t this totally amazing? Scientists can use skin cells and turn them into brain cells and study the function of those cells57. Induced pluripotent stem cells obtained from humans can also offer results fairly quickly, allowing scientific advances to emerge more rapidly than by obtaining and using brain tissue58. They can also allow for multiple sets of questions to be answered at once, by introducing new genes, environmental factors, or both into the mix58.
This process does not replace the important resource of studying cells directly from brains of people with autism. However, there is just not enough brain tissue to use so scientists are exploring other options. In fact, researchers use a combination of brain tissue analysis and neural stem cells to identify specific molecules in brain development in those with ASD, and the function of those molecules by inserting those molecules into neural stem cells59. It has validated the role of some small molecules in both brain development in ASD, and the continued production of cells in the brain including those that share information and those that have more support roles59. Using cells as a model for autism has huge potential for better understanding of the basic biology of ASD, which will lead to better individualized interventions.
Genetics and intermediate level phenotypes: endophenotypes
Mark Shen MRI” data-medium-file=”https://autismsciencefoundation.files.wordpress.com/2017/12/markshen-unc.png?w=296&h=142?w=300″ data-large-file=”https://autismsciencefoundation.files.wordpress.com/2017/12/markshen-unc.png?w=296&h=142?w=500″> Extra-axial fluid in the brain of a child with ASD (right). Credit: Mark Shen, University of North Carolina at Chapel Hill
Scientists are spending more and more time identifying the endophenotypesof autism to better understand autism subgroups. Endophenotypes are groups of biological markers that might serve in better diagnosis, but are not autism. They are usually tied to genetics. These markers are incredibly important in both understanding the development of autism and serving as objective markers for treatment protocols. They can include brain activity, brain structure, or behaviors like language delay.
This year researchers explored some of these endophenotypes not as a single biomarker, but things that could be added together to create a profile of probability of a diagnosis. The Baby Siblings Research Consortium, a group that tracks infants from high-risk families through diagnosis and adolescence, has made great advances this year. For example, early language abilities, especially understanding language, emerged as a strong endophenotype60. In fact, persistent language delay predicted ASD outcome in an independent group of kids61, reinforcing its use as an intermediate phenotype. In addition, changes in brainwave patterns, even as early as three months of age, years before a diagnosis, were shown to be a strong predictor of diagnosis62and even abnormal brainwave patterns without full blown seizure activity is common in those with ASD63. Measuring brainwave pattern through a technique called electroencephalography or EEG is viable in a number of different common clinical situations and might be used in larger scale studies besides those with high genetic risk for ASD. In addition to studying brain function, features of brain structure were also identified. Multiple replications in different samples showed a significant increase in extra axial fluid around the brains of children with autism64. This could be a marker of a biologically distinct subtype of autism. Researchers continue to study endophenotypes as markers of change, improvement, or prediction.
Better outcome measures for better treatment
While progress is being made in biological features of autism which can stratify different subgroups of autism, or measure biological differences across time through treatment to measure change, they are not yet ready for use in clinical settings. Unfortunately, the behavioral measures that scientists have used so far to measure treatment response were either developed for people without ASD, or those that were not intended to differences across time. Researchers have been working for years on developing measures which are based on clinician observation to document progress and can detect these improvements. This year, the BOSCC, or Brief Observation of Social Communication Change was validated65and is now being used in ongoing research studies. It is also important to note that this year, interventions were delivered in even a wider choice of settings. Preliminary results showed that Early Intense Behavioral Intervention, based on the principles of ABA, improved cognitive functioning and allowed for less restrictive school placements66. ABA or applied behavioral analysis, should be considered more as a set of guiding principles delivered by trained clinicians, rather than one specific practice. Importantly the interventions were delivered by trained community providers, which is where most kids and autistic adults receive help. Moving some of these interventions into the schools can be challenging, but progress was made this year. At the risk of sounding like a broken record, teachers are overworked, underpaid, sometimes unappreciated, but in most cases, they want to do what is best for their students. There can be wide variability in how teachers implement what they have learned during training into a chaotic classroom with students of varying needs. Despite this, teachers have taken on interventions that focus on things like transitions in elementary classrooms, with some success67. This has required developing outcomes based not just on child outcome, but teacher behaviors as well. Going forward, not only is there need for new measures, but also continuing partnerships from clinic to real world practice68.
Autism, employment, and suicide
Autism originates in childhood, and researchers have focused a lot of their time understanding autism in childhood. There is still much to be learned, including predicting adult outcomes based on features of autism in childhood, better understanding of the early signs and symptoms for better understanding of autism across the lifespan, the role of early intervention on longer term trajectories, and how early biological markers can help in better diagnosis and understanding of symptoms.
Photo courtesy of Extraordinary Ventures
An increasing number of researchers are focusing their efforts on factors that affect the quality of life, rather than autistic symptomatology, of individuals at all ages. This year, the International Society for Autism Research provided support for the development of a policy brief on employment in people with autism, and some of the early results support the need for a strengths based approach to employing people on the spectrum69. They noted that most of the literature has used approaches to manage symptoms in the workplace or help individuals with autism reduce problem behaviors.
An alternative approach could be to identify strengths of individuals and use those strengths productively69. In addition, based on feedback from families and individuals on the spectrum70, researchers are using employment as an outcome measure for interventions including cognitive behavioral therapy71 and other therapies72.
Scientists are just starting to understand a taboo subject in autism that typically occurs in adolescence to early adulthood: suicide. A recent review revealed that most of the research on suicide in autism has been conducted in the last five years73. In one study, those with social communication deficits rather than an autism diagnosis showed a higher rate of suicidal ideation74. Social communication deficits as a core symptom of autism, could be the target of interventions to prevent suicidal ideation. In other studies, those with autism have been shown to have up to a 66% rate of suicidal ideation and 30% rate of suicide attempt75. Unfortunately, there are still no good diagnostic tools to detect suicidal thoughts in those with autism75. Specific to the autism community, unmet care needs rose as an important risk factor for suicidal ideation76. Data gathered about people who are hospitalized for psychiatric problems (psychiatric inpatients) show that depression and anxiety are important risk factors for suicidal ideation and those conditions should be treated in this population77.
Lessons from the autism inpatient collection
Psychiatric inpatients have as high as a 10% rate of an ASD78, and because of their unique features, those with severe behaviors are often the least likely to be researched79. Those with more severe behaviors tend to be underrepresented in autism research and their needs are likely misunderstood80 Their needs are often ignored, but thanks to the Autism Inpatient Collection (AIC) (https://iancommunity.org/aic), a research study which includes many of the larger autism inpatient populations, this is changing. By studying autism inpatients, researchers have the opportunity to examine issues relating to those whose minimal language, intellectual disability, and self-injury requiring hospitalization. Not surprisingly, rates of documented self-injurious behaviors are higher in a hospital setting than in a community setting because that is why patients are there. In the AIC, those who exhibited self-injury at home and in the hospital had lower IQ and more severe repetitive behavior scores, but no differences in autism severity81. On the other hand, behaviors such as irritability and hyperactivity are also associated with shorter sleep in hospital settings, which is also not influenced by autism severity scores82.
The lack of connection between autism severity, sleep, and self-injury suggests that self-injury and shorter sleep duration may represent a different dimension of autism rather than a feature of autism itself.
Treatments from plants, pills, and the classroom:
One of the hottest topics this year has been the approval of a cannabis drug to treat seizures in people with a rare genetic mutation called Dravet Syndrome. The drug, called Epidiolex, is a high concentration of cannabidiol or CBD, and was shown effective in clinical trials and its approval, and also opened the doors to study and demonstrate the efficacy in treating seizures of people with a multitude of syndromes besides Dravet83,84. Cannabidiol, the main ingredient in Epidiolex, is obtained from the marijuana plant, but contains no THC or hallucinogenic cannabinoids. Nevertheless, the approval of this drug, together with marijuana legalization initiatives in several states, has elevated the discussion on the use of medical marijuana in the treatment of autism. While the effects of CBD for treatment of seizures is more established, scientists are currently studying the effectiveness of the cannabis plant or other cannabis extracts in treating core symptoms of autism85.
In addition to cannabis, in 2018 researchers explored additional pharmaceutical treatments. They include drugs that were previously used to treat other conditions. For example, bumetanide, a drug used to treat kidney failure, showed positive responses on eye contact in people with autism86. It also alleviated over activation of the amygdala,86which is thought to be a neurobiological feature of ASD and anxiety.
Kids with autism have more neurons in the amygdala, but by adolescence, they have fewer. Figure courtesy of Thomas Avino at UC Davis
The amygdala is known as the fear center, and ties emotional values onto different stimuli, making it a key area of interest in ASD. In fact, a groundbreaking study of autism brain tissue from individuals of multiple ages showed that the while kids with autism started out with a higher number of neurons in the amygdala, around adolescence, they dropped to lower than those who were neurotypical87. This suggests that the excess of cells in the amygdala early on cause this region to be too excited, and possibly leads to toxicity87. This important finding of a developmental shift in the amygdala in adolescence supports the amygdala as a focus for future treatments. In addition, simvastatin, a drug used to treat high cholesterol, also showed positive effects in two different studies of autism88,89.
But not all effective treatments for autism come in the form of a pill or an oil. Behavioral based interventions that were once used only for preschoolers, are now being deployed in classroom settings. Thanks to patient, supportive researchers who worked closely with dedicated, hardworking teachers, the teachers delivered behavioral interventions that resulted in improved outcomes in students67,90. These improvements were not easy – teachers must be trained and be willing to incorporate the intervention into the classroom and receive instruction.
Tristram Smith, one of the researchers involved in a study of kids in low resourced schools,67passed away in 2018. His compassion and dedication to the field is sorely missed. He was crucial in helping to show that teachers and interventionists who work together can make a difference for school-aged kids with ASD.
Through the years
If money and time were no object, there would be more longitudinal studies in ASD. Longitudinal studies in autism track each person on an individual basis from before they received a diagnosis through adulthood. Longitudinal research is able to not just look at differences between those with autism and without, but also look at the trajectories of behavior across a few years to a few decades. These studies can describe features of autism or be predictive in helping identify subgroups that respond to treatment or identify early features to predict later ones. A collaboration between multiple research groups has tracked a group of people with autism from age 2 to now age 19 and identified common and distinct patterns of behavioral development, illustrating what can happen as children become adults. It shows that, overall, there is improvement in some symptoms of autism including social communication. However, this improvement was somewhat dependent on language ability91. While this is not always the case, it shows that there are always lifelong opportunities to learn, and improvements can be seen in people with autism across the lifespan. Cognitive abilities in childhood seem to play a big role in cognitive function in adulthood, although many children show academic challenges even with normal to high IQ92. Even in younger children, there is great variability in the trajectories of adaptive behavior, which is a measure of functioning in individuals with autism. Some improve over time, and some decline93. Understanding the differences between people with autism whose symptoms stay stable vs. those that decline may be critically important to future diagnosis and intervention studies. These studies emphasize the importance of early intervention, a tailored individualized approach, and also academic and social support across the lifespan.
What it all means
There were a number of exciting advances in understanding autism in 2018. Researchers made progress in identifying subgroups of ASD, defining biological markers, and developing interventions. There were also studies that demonstrate that while autism is a spectrum itself, it is also part of a bigger spectrum of neurodevelopmental disorders from anxiety to ADHD to OCD. Therefore, the approaches to these other conditions may be applicable to ASD. In addition, there may be more similarities than differences in the biological features of these conditions.
Autism is distinct from other diagnoses, and despite the vast differences in symptom presentation, onset, and severity, findings call for improved access to services across all intellectual abilities and through different generations.
Thank you
The advances in scientific understanding of autism this year are because families trust research with their money, their time, and their expertise. Thank you to everyone who conducted research into autism, those who participated in a research study or contributed financially.
References:
Davignon MN, Qian Y, Massolo M, Croen LA. Psychiatric and Medical Conditions in Transition-Aged Individuals With ASD.Pediatrics. 2018;141(Suppl 4):S335-S345.
Septier M, Peyre H, Amsellem F, et al. Increased risk of ADHD in families with ASD. Eur Child Adolesc Psychiatry. 2018.
Chen MH, Hsu JW, Huang KL, et al. Risk and coaggregation of major psychiatric disorders among first-degree relatives of patients with bipolar disorder: a nationwide population-based study. Psychol Med. 2018:1-8.
Cheng CM, Chang WH, Chen MH, et al. Co-aggregation of major psychiatric disorders in individuals with first-degree relatives with schizophrenia: a nationwide population-based study. Mol Psychiatry. 2018;23(8):1756-1763.
Karalunas SL, Hawkey E, Gustafsson H, et al. Overlapping and Distinct Cognitive Impairments in Attention-Deficit/Hyperactivity and Autism Spectrum Disorder without Intellectual Disability. J Abnorm Child Psychol. 2018;46(8):1705-1716.
Berenguer C, Rosello B, Colomer C, Baixauli I, Miranda A. Children with autism and attention deficit hyperactivity disorder. Relationships between symptoms and executive function, theory of mind, and behavioral problems. Res Dev Disabil. 2018;83:260-269.
Hollocks MJ, Lerh JW, Magiati I, Meiser-Stedman R, Brugha TS. Anxiety and depression in adults with autism spectrum disorder: a systematic review and meta-analysis. Psychol Med. 2018:1-14.
Shephard E, Bedford R, Milosavljevic B, et al. Early developmental pathways to childhood symptoms of attention-deficit hyperactivity disorder, anxiety and autism spectrum disorder. J Child Psychol Psychiatry. 2018.
Neuhaus E, Bernier RA, Tham SW, Webb SJ. Gastrointestinal and Psychiatric Symptoms Among Children and Adolescents With Autism Spectrum Disorder. Front Psychiatry. 2018;9:515.
Kogan MD, Vladutiu CJ, Schieve LA, et al. The Prevalence of Parent-Reported Autism Spectrum Disorder Among US Children. Pediatrics.2018;142(6).
Karpur A, Lello A, Frazier T, Dixon PJ, Shih AJ. Health Disparities among Children with Autism Spectrum Disorders: Analysis of the National Survey of Children’s Health 2016. J Autism Dev Disord. 2018.
Candon MK, Barry CL, Marcus SC, et al. Insurance Mandates and Out-of-Pocket Spending for Children With Autism Spectrum Disorder. Pediatrics.2018.
Gandal MJ, Haney JR, Parikshak NN, et al. Shared molecular neuropathology across major psychiatric disorders parallels polygenic overlap. Science. 2018;359(6376):693-697.
Yu Q, He Z, Zubkov D, et al. Lipidome alterations in human prefrontal cortex during development, aging, and cognitive disorders. Mol Psychiatry. 2018.
Gandal MJ, Zhang P, Hadjimichael E, et al. Transcriptome-wide isoform-level dysregulation in ASD, schizophrenia, and bipolar disorder. Science. 2018;362(6420).
Brainstorm C, Anttila V, Bulik-Sullivan B, et al. Analysis of shared heritability in common disorders of the brain. Science. 2018;360(6395).
Pettersson E, Lichtenstein P, Larsson H, et al. Genetic influences on eight psychiatric disorders based on family data of 4 408 646 full and half-siblings, and genetic data of 333 748 cases and controls. Psychol Med. 2018:1-8.
De Rubeis S, Siper PM, Durkin A, et al. Delineation of the genetic and clinical spectrum of Phelan-McDermid syndrome caused by SHANK3 point mutations. Mol Autism. 2018;9:31.
Abbeduto L, Thurman AJ, McDuffie A, et al. ASD Comorbidity in Fragile X Syndrome: Symptom Profile and Predictors of Symptom Severity in Adolescent and Young Adult Males. J Autism Dev Disord. 2018.
Vismara LA, McCormick CEB, Shields R, Hessl D. Extending the Parent-Delivered Early Start Denver Model to Young Children with Fragile X Syndrome. J Autism Dev Disord. 2018.
Steinmetz AB, Stern SA, Kohtz AS, Descalzi G, Alberini CM. Insulin-Like Growth Factor II Targets the mTOR Pathway to Reverse Autism-Like Phenotypes in Mice. J Neurosci. 2018;38(4):1015-1029.
Wegiel J, Brown WT, La Fauci G, et al. The role of reduced expression of fragile X mental retardation protein in neurons and increased expression in astrocytes in idiopathic and syndromic autism (duplications 15q11.2-q13). Autism Res. 2018;11(10):1316-1331.
Parikshak NN, Swarup V, Belgard TG, et al. Genome-wide changes in lncRNA, splicing, and regional gene expression patterns in autism. Nature. 2016;540(7633):423-427.
Baio J, Wiggins L, Christensen DL, et al. Prevalence of Autism Spectrum Disorder Among Children Aged 8 Years – Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2014. MMWR Surveill Summ. 2018;67(6):1-23.
Schendel DE, Thorsteinsson E. Cumulative Incidence of Autism Into Adulthood for Birth Cohorts in Denmark, 1980-2012. JAMA. 2018;320(17):1811-1813.
Ozonoff S, Young GS, Brian J, et al. Diagnosis of Autism Spectrum Disorder After Age 5 in Children Evaluated Longitudinally Since Infancy. J Am Acad Child Adolesc Psychiatry. 2018;57(11):849-857 e842.
Harrop C, Jones D, Zheng S, Nowell SW, Boyd BA, Sasson N. Sex differences in social attention in autism spectrum disorder. Autism Res. 2018;11(9):1264-1275.
Harrop C, Jones D, Zheng S, Nowell S, Boyd BA, Sasson N. Circumscribed Interests and Attention in Autism: The Role of Biological Sex. J Autism Dev Disord. 2018;48(10):3449-3459.
Lai MC, Lombardo MV, Chakrabarti B, et al. Neural self-representation in autistic women and association with ‘compensatory camouflaging’. Autism. 2018:1362361318807159.
Lombardo MV, Auyeung B, Pramparo T, et al. Sex-specific impact of prenatal androgens on social brain default mode subsystems. Mol Psychiatry. 2018.
Quartier A, Chatrousse L, Redin C, et al. Genes and Pathways Regulated by Androgens in Human Neural Cells, Potential Candidates for the Male Excess in Autism Spectrum Disorder. Biol Psychiatry. 2018;84(4):239-252.
Cherskov A, Pohl A, Allison C, Zhang H, Payne RA, Baron-Cohen S. Polycystic ovary syndrome and autism: A test of the prenatal sex steroid theory. Transl Psychiatry. 2018;8(1):136.
Chen G, Jin Z, Li S, et al. Early life exposure to particulate matter air pollution (PM1, PM2.5 and PM10) and autism in Shanghai, China: A case-control study. Environ Int. 2018.
Kalkbrenner AE, Windham GC, Zheng C, et al. Air Toxics in Relation to Autism Diagnosis, Phenotype, and Severity in a U.S. Family-Based Study. Environ Health Perspect. 2018;126(3):037004.
Mandy W, Pellicano L, St Pourcain B, Skuse D, Heron J. The development of autistic social traits across childhood and adolescence in males and females. J Child Psychol Psychiatry. 2018;59(11):1143-1151.
La Buissonniere-Ariza V, Wood JJ, Kendall PC, et al. Presentation and Correlates of Hoarding Behaviors in Children with Autism Spectrum Disorders and Comorbid Anxiety or Obsessive-Compulsive Symptoms. J Autism Dev Disord. 2018;48(12):4167-4178.
Pagalan L, Bickford C, Weikum W, et al. Association of Prenatal Exposure to Air Pollution With Autism Spectrum Disorder. JAMA Pediatr. 2018.
Brown AS, Cheslack-Postava K, Rantakokko P, et al. Association of Maternal Insecticide Levels With Autism in Offspring From a National Birth Cohort. Am J Psychiatry. 2018:appiajp201817101129.
Croen LA, Qian Y, Ashwood P, et al. Family history of immune conditions and autism spectrum and developmental disorders: Findings from the study to explore early development.Autism Res. 2018.
Rubenstein E, Young JC, Croen LA, et al. Brief Report: Maternal Opioid Prescription from Preconception Through Pregnancy and the Odds of Autism Spectrum Disorder and Autism Features in Children. J Autism Dev Disord. 2018.
Wimberley T, Agerbo E, Pedersen CB, et al. Otitis media, antibiotics, and risk of autism spectrum disorder. Autism Res. 2018;11(10):1432-1440.
Curtin P, Austin C, Curtin A, et al. Dynamical features in fetal and postnatal zinc-copper metabolic cycles predict the emergence of autism spectrum disorder.Sci Adv. 2018;4(5):eaat1293.
Schwede M, Nagpal S, Gandal MJ, et al. Strong correlation of downregulated genes related to synaptic transmission and mitochondria in post-mortem autism cerebral cortex. J Neurodev Disord. 2018;10(1):18.
An JY, Lin K, Zhu L, et al. Genome-wide de novo risk score implicates promoter variation in autism spectrum disorder. Science.2018;362(6420).
Woodbury-Smith M, Scherer SW. Progress in the genetics of autism spectrum disorder. Dev Med Child Neurol. 2018;60(5):445-451.
Woodbury-Smith M, Paterson AD, O’Connor I, et al. A genome-wide linkage study of autism spectrum disorder and the broad autism phenotype in extended pedigrees. J Neurodev Disord. 2018;10(1):20.
Brandler WM, Antaki D, Gujral M, et al. Paternally inherited cis-regulatory structural variants are associated with autism. Science.2018;360(6386):327-331.
Williams SM, An JY, Edson J, et al. An integrative analysis of non-coding regulatory DNA variations associated with autism spectrum disorder. Mol Psychiatry. 2018.
Werling DM, Brand H, An JY, et al. An analytical framework for whole-genome sequence association studies and its implications for autism spectrum disorder. Nat Genet. 2018;50(5):727-736.
Willingham E. Optimism, confusion greet federal fast track for autism drug. Spectrum News; 2018.
Berg EL, Copping NA, Rivera JK, et al. Developmental social communication deficits in the Shank3 rat model of phelan-mcdermid syndrome and autism spectrum disorder. Autism Res. 2018;11(4):587-601.
Hulbert SW, Bey AL, Jiang YH. Environmental enrichment has minimal effects on behavior in the Shank3 complete knockout model of autism spectrum disorder. Brain Behav. 2018;8(11):e01107.
Qin L, Ma K, Wang ZJ, et al. Social deficits in Shank3-deficient mouse models of autism are rescued by histone deacetylase (HDAC) inhibition. Nat Neurosci. 2018;21(4):564-575.
Dalla Vecchia E, Mortimer N, Palladino VS, et al. Cross-species models of attention-deficit/hyperactivity disorder and autism spectrum disorder: lessons from CNTNAP2, ADGRL3, and PARK2.Psychiatr Genet. 2018.
Jung H, Park H, Choi Y, et al. Sexually dimorphic behavior, neuronal activity, and gene expression in Chd8-mutant mice. Nat Neurosci.2018;21(9):1218-1228.
Zerbi V, Ielacqua GD, Markicevic M, et al. Dysfunctional Autism Risk Genes Cause Circuit-Specific Connectivity Deficits With Distinct Developmental Trajectories. Cereb Cortex. 2018;28(7):2495-2506.
DeRosa BA, El Hokayem J, Artimovich E, et al. Convergent Pathways in Idiopathic Autism Revealed by Time Course Transcriptomic Analysis of Patient-Derived Neurons. Sci Rep. 2018;8(1):8423.
Williams M, Prem S, Zhou X, et al. Rapid Detection of Neurodevelopmental Phenotypes in Human Neural Precursor Cells (NPCs). J Vis Exp. 2018(133).
Nguyen LS, Fregeac J, Bole-Feysot C, et al. Role of miR-146a in neural stem cell differentiation and neural lineage determination: relevance for neurodevelopmental disorders. Mol Autism.2018;9:38.
Marrus N, Hall LP, Paterson SJ, et al. Language delay aggregates in toddler siblings of children with autism spectrum disorder. J Neurodev Disord. 2018;10(1):29.
Henry L, Farmer C, Manwaring SS, Swineford L, Thurm A. Trajectories of cognitive development in toddlers with language delays. Res Dev Disabil. 2018;81:65-72.
Bosl WJ, Tager-Flusberg H, Nelson CA. EEG Analytics for Early Detection of Autism Spectrum Disorder: A data-driven approach. Sci Rep. 2018;8(1):6828.
Capal JK, Carosella C, Corbin E, Horn PS, Caine R, Manning-Courtney P. EEG endophenotypes in autism spectrum disorder. Epilepsy Behav. 2018;88:341-348.
Shen MD, Nordahl CW, Li DD, et al. Extra-axial cerebrospinal fluid in high-risk and normal-risk children with autism aged 2-4 years: a case-control study. Lancet Psychiatry. 2018;5(11):895-904.
Kim SH, Grzadzinski R, Martinez K, Lord C. Measuring treatment response in children with autism spectrum disorder: Applications of the Brief Observation of Social Communication Change to the Autism Diagnostic Observation Schedule. Autism. 2018:1362361318793253.
Waters CF, Amerine Dickens M, Thurston SW, Lu X, Smith T. Sustainability of Early Intensive Behavioral Intervention for Children With Autism Spectrum Disorder in a Community Setting. Behav Modif. 2018:145445518786463.
Iadarola S, Shih W, Dean M, et al. Implementing a Manualized, Classroom Transition Intervention for Students With ASD in Underresourced Schools. Behav Modif. 2018;42(1):126-147.
Bal VH, Hendren RL, Charman T, et al. Considerations from the 2017 IMFAR Preconference on Measuring Meaningful Outcomes from School-Age to Adulthood. Autism Res. 2018;11(11):1446-1454.
Scott M, Milbourn B, Falkmer M, et al. Factors impacting employment for people with autism spectrum disorder: A scoping review. Autism.2018:1362361318787789.
Anderson KA, Sosnowy C, Kuo AA, Shattuck PT. Transition of Individuals With Autism to Adulthood: A Review of Qualitative Studies. Pediatrics.2018;141(Suppl 4):S318-S327.
Eack SM, Hogarty SS, Greenwald DP, et al. Cognitive enhancement therapy for adult autism spectrum disorder: Results of an 18-month randomized clinical trial. Autism Res. 2018;11(3):519-530.
Hatfield M, Falkmer M, Falkmer T, Ciccarelli M. Effectiveness of the BOOST-A online transition planning program for adolescents on the autism spectrum: a quasi-randomized controlled trial. Child Adolesc Psychiatry Ment Health. 2017;11:54.
Veenstra-VanderWeele J. Recognizing the Problem of Suicidality in Autism Spectrum Disorder. J Am Acad Child Adolesc Psychiatry. 2018;57(5):302-303.
Culpin I, Mars B, Pearson RM, et al. Autistic Traits and Suicidal Thoughts, Plans, and Self-Harm in Late Adolescence: Population-Based Cohort Study. J Am Acad Child Adolesc Psychiatry. 2018;57(5):313-320 e316.
Cassidy SA, Bradley L, Bowen E, Wigham S, Rodgers J. Measurement properties of tools used to assess suicidality in autistic and general population adults: A systematic review. Clin Psychol Rev. 2018;62:56-70.
Cassidy S, Bradley L, Shaw R, Baron-Cohen S. Risk markers for suicidality in autistic adults. Mol Autism. 2018;9:42.
Horowitz LM, Thurm A, Farmer C, et al. Talking About Death or Suicide: Prevalence and Clinical Correlates in Youth with Autism Spectrum Disorder in the Psychiatric Inpatient Setting. J Autism Dev Disord. 2018;48(11):3702-3710.
Tromans S, Chester V, Kiani R, Alexander R, Brugha T. The Prevalence of Autism Spectrum Disorders in Adult Psychiatric Inpatients: A Systematic Review. Clin Pract Epidemiol Ment Health. 2018;14:177-187.
Siegel M. The Severe End of the Spectrum: Insights and Opportunities from the Autism Inpatient Collection (AIC). J Autism Dev Disord. 2018;48(11):3641-3646.
Stedman A, Taylor B, Erard M, Peura C, Siegel M. Are Children Severely Affected by Autism Spectrum Disorder Underrepresented in Treatment Studies? An Analysis of the Literature. J Autism Dev Disord. 2018.
Handen BL, Mazefsky CA, Gabriels RL, et al. Risk Factors for Self-injurious Behavior in an Inpatient Psychiatric Sample of Children with Autism Spectrum Disorder: A Naturalistic Observation Study. J Autism Dev Disord. 2018;48(11):3678-3688.
Sannar EM, Palka T, Beresford C, et al. Sleep Problems and Their Relationship to Maladaptive Behavior Severity in Psychiatrically Hospitalized Children with Autism Spectrum Disorder (ASD). J Autism Dev Disord. 2018;48(11):3720-3726.
Szaflarski JP, Bebin EM, Cutter G, et al. Cannabidiol improves frequency and severity of seizures and reduces adverse events in an open-label add-on prospective study. Epilepsy Behav. 2018.
Devinsky O, Verducci C, Thiele EA, et al. Open-label use of highly purified CBD (Epidiolex(R)) in patients with CDKL5 deficiency disorder and Aicardi, Dup15q, and Doose syndromes. Epilepsy Behav. 2018;86:131-137.
Aran A, Cassuto H, Lubotzky A, Wattad N, Hazan E. Brief Report: Cannabidiol-Rich Cannabis in Children with Autism Spectrum Disorder and Severe Behavioral Problems-A Retrospective Feasibility Study. J Autism Dev Disord. 2018.
Hadjikhani N, Asberg Johnels J, Lassalle A, et al. Bumetanide for autism: more eye contact, less amygdala activation. Sci Rep. 2018;8(1):3602.
Avino TA, Barger N, Vargas MV, et al. Neuron numbers increase in the human amygdala from birth to adulthood, but not in autism. Proc Natl Acad Sci U S A. 2018;115(14):3710-3715.
Moazen-Zadeh E, Shirzad F, Karkhaneh-Yousefi MA, Khezri R, Mohammadi MR, Akhondzadeh S. Simvastatin as an Adjunctive Therapy to Risperidone in Treatment of Autism: A Randomized, Double-Blind, Placebo-Controlled Clinical Trial. J Child Adolesc Psychopharmacol. 2018;28(1):82-89.
Stivaros S, Garg S, Tziraki M, et al. Randomised controlled trial of simvastatin treatment for autism in young children with neurofibromatosis type 1 (SANTA). Mol Autism. 2018;9:12.
Morgan L, Hooker JL, Sparapani N, Reinhardt VP, Schatschneider C, Wetherby AM. Cluster randomized trial of the classroom SCERTS intervention for elementary students with autism spectrum disorder. J Consult Clin Psychol. 2018;86(7):631-644.
Bal VH, Kim SH, Fok M, Lord C. Autism spectrum disorder symptoms from ages 2 to 19 years: Implications for diagnosing adolescents and young adults. Autism Res. 2018.
Kim SH, Bal VH, Lord C. Longitudinal follow-up of academic achievement in children with autism from age 2 to 18. J Child Psychol Psychiatry. 2018;59(3):258-267.
Sacrey LR, Zwaigenbaum L, Bryson S, et al. Developmental trajectories of adaptive behavior in autism spectrum disorder: a high-risk sibling cohort. J Child Psychol Psychiatry. 2018.
Niemi MEK, Martin HC, Rice DL. et al. Common genetic variants contribute to risk of rare severe neurodevelopmental disorders. Nature. 2018; 562(7726):268-271.
by Alycia Halladay, PhD, Chief Science Officer and The Scientific Advisory Board of ASF
The COVID-19 pandemic upended the lives of families around the world, but autism families were dealt an even harsher hand. Autism families rely on frequent in-person therapies such as speech, occupational therapy and applied behavioral analysis. Most often, these services are provided in schools or clinics; the pandemic has disrupted or eliminated treatment in both settings, resulting in further isolation of people with ASD and their families1,2. This isolation manifests as increased screen time, reduced exercise and decreased social interaction. In addition, comorbidities have heightened the risk of COVID hospitalization, a fear that weighs heavily on the minds of autism parents3,4.
Surveys of families affected with ASD link high stress levels to the strain of constant care of individuals with ASD and concerns about the person with ASD becoming ill3. These concerns increase with severity of ASD symptoms. According to caregivers, those who lost access to school-based services are the most affected. Fear of exposure to COVID-19 discouraged families from taking needed respite care or eliminated it as a possibility. While concerns about the health of the person with ASD generate the greatest stress, financial concerns and worries about the health of all family members3 greatly compound it. In fact, compared to neurotypical children and adolescents, those with autism have a higher rate of emotional problems and conduct problems and showed reduced sociability during the shutdown5.
One of the hardest hit populations may be those with profound autism, severe behaviors and intellectual disabilities. A survey of families with children with rare genetic forms of ASD (who typically show more severe behaviors) reveals that almost half of those surveyed lost school-provided academic services and not all were able to re-access them via telehealth. However, of those who lost medical services, about 50% were able receive services via telehealth, and many hoped to continue telehealth after the pandemic had resolved6. Things were especially dire for families mid-shutdown, and these families should be followed up to see what accommodations worked and which did not.
1 in 54
In the midst of the pandemic, the CDC released data that showed a small increase in the prevalence of autism in 8 year olds7. Some of this change might be attributed to a rise in recognized prevalence of ASD in black children, which has been historically low due to under ascertainment. A similar trend was also seen in 4 year olds in non-white racial and ethnic groups8. While less disparity in recognition and diagnosis in non-white children is good news, the increase in prevalence of ASD in children of color is a call to action for communities to ensure access to care for all children. Another CDC analysis using the ADDM methodology showed that 25% of kids noted to have ASD using record review are not actually diagnosed with ASD; half of those were not receiving any services9. What is causing this increase in prevalence? Certainly, better surveillance is one factor, but there is increasing evidence that genetic and environmental interactions may be contributing to an ASD diagnoisis10,11.
Black Lives Matter
With the murder of George Floyd earlier this year, racial tensions in the United States engendered an international re-awakening and re-ignited awareness of racism and systemic discrimination. This is true in many areas of sociology and psychology and autism is no exception. While the gap in diagnosis between black and white children is narrowing, it still persists. There is a higher risk for non-white children to be missed and not receive an appropriate diagnosis9. The diagnostic experiences of black children was documented in an in-depth analysis of families who are involved with the AGRE database. Their age of diagnosis is higher as compared to white children, despite the age of parent concern being similar. The delay is not due to lack of insurance or presence of intellectual disability, the latter usually lowers the age of diagnosis due to more recognizable symptoms12. This significant delay in formal diagnosis robs non-white children of the opportunity for early intervention. A systematic review summarizing decades worth of research also highlighted fewer opportunities for access to care, a higher proportion of unmet service needs and less access to specialized medical, educational and community services for children of color, when compared to white families13. Not surprisingly, African-American parents also have documented higher levels of parenting stress compared to white families14.
Late this year, a study reported that a visually-based screening tool for Hispanic families (and potentially others) worked better in that population than traditional tools15. Other systematic changes need to occur in autism research to create greater diversity, including recruiting more diverse scientists and physicians into autism treatment and research, and developing and maintaining programs to keep them working with families with ASD16.
Earlier detection and diagnosis
The year 2020 saw renewed efforts to find innovative approaches to improve diagnosis for all children. Most of these studies took place with infants with a high probability of diagnosis because they have diagnosed older siblings. Several have demonstrated the promise of EEG – electroencephalography – as a way to find biomarkers that predict autism and reveal further understanding of how the brains of infants and toddlers work. For example, new studies found that toddlers who show late signs of ASD have lower levels of electrical communication in the frontal and middle parts of the brain17,18. Differences in infant brain activity, as well as particular electrical signals, also serve to predict learning ability and later markers of intelligence in ASD19,20. In addition, assessing certain measures in persons with autism (proband) may help predict the probability of autism or the severity of its symptoms in younger siblings, specifically adaptive behavior, communication and language21. Also, early observations of how babies look at and respond to their mothers and how they match expressions and respond to mothers’ voices are an indicator of ASD risk. These markers could be used as targets to improve language and communication21-23.
Understanding heritability is also key to predicting an autism diagnosis. Early this year, a scientific analysis examined sperm of fathers with kids with ASD and the presence of de-novo mutations. These de-novo mutations appear in the person with ASD but not in the blood of either parent and therefore the origin of these mutations is elusive. A significant proportion of fathers with kids with de-novo mutations and autism had mutations in their sperm, but not their blood. This is called a somatic mutation because it is not found in all tissues of the body24. While still in early days, these findings suggest a pre-conception marker for autism probability may potentially be found in sperm24. It’s also important to note that not all of the de-novo mutations could be found in fathers’ sperm.
The largest analysis of genes associated with autism published this year not only identified 102 genes that significantly contributed to autism risk, but also noted that some are associated with neurodevelopmental disorders in general, including intellectual disability, while others were specific to ASD25. A separate commentary pointed out that across publications in ASD genetics, there are very few, if any genes, specific to autism26. Many families have asked why genetic analysis is necessary since genes are biologically innate and cannot be changed. A recent analysis found that 12% of autism cases resulted from a pathogenic gene found upon genetic testing. Families that have children with genetic mutations often join together for support and advocacy and may receive opportunities to participate in clinical trials that target their specific genetic mutation27.
A newer area of scientific genome study involves not DNA, but epigenomes, which are chemical modifications to DNA that serve to turn genes on and off. Cord blood obtained from infants who develop autism has a different methylation profile than that of those who do not develop ASD28, suggesting epigenetic assays that measure modifications of DNA should be utilized to understand the probability of a diagnosis as well, especially in specific phenotypes29. It is also becoming clearer that those with a strong genetic familial influence may show different risk factors than those with no family history. For example, the influence of paternal age and gestational obesity and metabolic disorders on likelihood of having a child with ASD differs based on family history30,31.
Heritability in ASD also includes non-genetic factors, including exposures of parents and grandparents. A preliminary analysis showed a slightly increased likelihood of ASD in frequent marijuana users32, possibly through changes in sperm, but that clearly does not explain all of the causes of ASD. In addition, low neonatal vasopressin levels were predictive of an ASD diagnosis in a small cohort. Other environmental factors known to be associated with ASD, such as air pollution, were studied in animal models. For example, the offspring of pregnant mice placed near roadway pollution exposures in California were found to have neurodevelopmental delays and social communication deficits33, further demonstrating the need to reduce air pollution to improve the health of children worldwide. The first study of the heritability of ASD across generations was explored this year, using subjects from the Swedish National Registry. In this study, researchers determined an elevated rate of autism in children of siblings with ASD. This is the first study to document the rate of ASD across generations, although more work needs to be done to understand this “next generation”33. Research along these lines has also shown differences in brain function in undiagnosed females with a family history of ASD, which may be passed on to later generations34.
Skin cells may lead to new options
The brain is the most important organ to study in ASD, but unfortunately not enough brain tissue exists for all new exciting and potentially revolutionizing scientific studies. That’s why it is important to learn about the Autism BrainNet which works to make sure families understand why brain tissue donation is so important. However, hanks to work by scientists across the world in different fields of research, ASD scientists can now use cells from different parts of the body, and, by adding chemicals and conducting genetic manipulations, turn those cells into brain cells to be studied. These initial cells can come from blood, teeth, the nose, or skin35. Because they are “induced” into becoming brain cells, they are called iPSCs or “induced pluripotent stem cells”. Although they aren’t true brain cells, they can be used to understand the brains of people with ASD, both with and without known genetic mutations, in the hopes of developing more targeted interventions. In fact, as more and more of the cells grow together, they connect, attach and grow in ways that have the shape of “mini-brains”36. These cells are now being used in experimental settings to understand how the brain connects, and to screen different compounds for treatment37,38.
Sex and Gender Differences
Sex differences in the way autism features and symptoms present have traditionally been hard to measure – the M/F disparity in diagnosis itself means that fewer females participate in research studies. There has been concern that diagnostic instruments may be biased and not pick up as many girls as boys. However by using a collection of databases across the world with over 9,000 people included, controlling for age and cognitive ability , scientists found that the standard screening and diagnostic instruments are not biased towards boys compared to girls39,40. Looking at particular age ranges, boys do seem to have more frequent restrictive and repetitive behavior earlier than their female counterparts, with girls showing more of these behaviors in adolescence39.
Another theory that might better illuminate the disparity in diagnosis is the idea that females may be protected against an autism diagnosis by genetic, environmental or other factors, or multiple factors working together. Several studies, including the largest one published this year25, confirm that females carry more genetic mutations across the genome compared to males. This suggests that females can tolerate more genetic mutations than males without showing symptoms41, supporting the hypothesis of the “female protective effect.”
Since they carry a higher level of risk factors, why the lower rate of diagnosis in females? One study using a cohort of younger siblings of individuals with ASD examined hormone levels at birth. While there were no differences overall, younger infant siblings with an older sister with ASD had a stronger relationship between many hormones found at birth and autism symptoms42. This effect has also been seen in other studies, and is suggestive of a differential role of genetic and environmental influences in siblings of females compared to males. More research is obviously needed. While they may explain male and female differences in the expression of features, these subtle differences, like improved sociability and camouflaging in females, do not count for the disparities in diagnosis between males and females43.
Cognitive and Verbal Abilities:
There has been great debate over the importance of language and cognitive abilities in people with ASD, as it may influence access to services. There is now more evidence that those with low cognitive ability or minimal language may constitute a subgroup of those with ASD that need a different approach. The patterns of brain activity in people with ASD with minimal verbal ability44,45 and heritability in those with decreased cognitive ability is, in fact, different than those with normal language function and ASD46.
How you define a good outcome and how a family perceives “success” depends significantly on cognitive ability. Families of those with lower cognitive ability consider a good outcome to be possessing adaptive skills above that of an 8-year-old, participating in activities outside of the home and engaging with social contacts outside of the family. Those with a higher cognitive ability define a good outcome as being employed (if they want to be), living independently and having at least one true friend. Things that influence good outcome in this group are fewer mental health problems and measures of happiness47. Mental health issues, like anxiety, present very differently across people with differing IQs and while several studies have linked higher IQ to higher levels of anxiety48,49, it may be that measures of anxiety are not sufficient in those with intellectual disability47.
Anxiety and Sleep
Families and individuals with ASD describe anxiety as one of the most serious problems facing people with autism. Anxiety occurs in as high as 80% of people with normal to high IQ, but it’s unclear what the prevalence is in those with lower IQ48. Cognitive Behavioral Therapy (CBT) has long been used as a treatment for anxiety symptoms, including in people with autism, but it may not be appropriate for those with lower IQs. While a large Cochrane review of CBT shows a mild level of improvement across studies50, more recent studies show larger improvements in community care settings51, and in young children and adolescents52,53. These may be particularly helpful for those with comorbid ADHD and anxiety in ASD54.
Sleep is also often highly disrupted in people with autism. This year, a study reported that the growth of the hippocampus in infancy is different in those with ASD and sleep issues compared to those without sleep issues55. This is the first study to show a specific biomarker for later sleep difficulties in infants – paving the way to more effective sleep therapies.
New Interventions and Telehealth
As new autism genes are identified (thanks to larger sample sizes and new sequencing techniques) scientists are moving quickly to create animal models with these mutations in order to understand the functions of the genes and ultimately, develop targeted interventions. The goal of these treatments is a reversal of any impairments in behavioral features of ASD like social interaction or vocalizations. These models can also show changes in brain structure or connection between neurons, which may also be altered by a treatment. In one model system, the target of intervention was the tau protein, which is also responsible for Alzheimer’s Disease. Knocking down tau alleviated symptoms of ASD in young mice54, and could possibly reduce cognitive declines in people with ASD and dementia. In another autism mouse model that knocks out the neuroligin protein, scientists found that a new cancer drug reversed neurobiological and behavioral symptoms associated with autism56. This compound could move to clinical trials in the coming years.
Studies of pandemic-induced telehealth-based interventions are just starting to emerge. One method of telehealth called ECHO, has been used by autism researchers for years, and recent studies show that it is effective in helping train other doctors and disseminate knowledge. ECHO stands for “Extension for Community Healthcare Outcomes” and has been used to help train care providers to treat everything from blood disorders to diabetes to opiate addiction all over the world. A group of researchers is working to determine its efficacy in helping physicians treat families with ASD. An experimental study showed that it improved pediatrician knowledge57, which led to higher screening rate58.
Other methods of autism screening are also being used via telehealth, including the Systematic Observation of Red Flags, a screening instrument that involves observation of home video clips59. Even biological measures, such as attention to social scenes, have been adapted for online use60. Successfully implementing valid online screening tools is critical during the pandemic when many clinics are closed, and will also be useful after the pandemic to ease the burden on families of having to travel to a clinic for assessment61.
2020 was a year like no other, in that families and scientists were forced to pivot rapidly and adjust to the harsh realities of COVID-19, but scientific progress continued, and many of the new adaptations have opened new avenues to improve diagnosis, screening, and service delivery for people with ASD. Instead of returning to normal, scientists will take what was useful and helpful via telehealth as well as new technologies developed during this time. Now, scientists will move on to continue helping families mid- and post-pandemic building on what was learned and having a better sense of how to be prepared.help their other family members and themselves.
References:
1. Amaral DG, de Vries PJ. COVID-19 and Autism Research: Perspectives from Around the Globe. Autism Res. 2020;13(6):844-869.
2. Bellomo TR, Prasad S, Munzer T, Laventhal N. The impact of the COVID-19 pandemic on children with autism spectrum disorders. J Pediatr Rehabil Med. 2020.
3. Manning J, Billian J, Matson J, Allen C, Soares N. Perceptions of Families of Individuals with Autism Spectrum Disorder during the COVID-19 Crisis. J Autism Dev Disord. 2020.
4. Garcia JM, Lawrence S, Brazendale K, Leahy N, Fukuda D. Brief report: The impact of the COVID-19 pandemic on health behaviors in adolescents with Autism Spectrum Disorder. Disabil Health J. 2020:101021.
5. Nonweiler J, Rattray F, Baulcomb J, Happe F, Absoud M. Prevalence and Associated Factors of Emotional and Behavioural Difficulties during COVID-19 Pandemic in Children with Neurodevelopmental Disorders. Children (Basel). 2020;7(9).
6. Jeste S, Hyde C, Distefano C, et al. Changes in access to educational and healthcare services for individuals with intellectual and developmental disabilities during COVID-19 restrictions. J Intellect Disabil Res. 2020.
7. Maenner MJ, Shaw KA, Baio J, et al. Prevalence of Autism Spectrum Disorder Among Children Aged 8 Years – Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2016. MMWR Surveill Summ. 2020;69(4):1-12.
8. Shaw KA, Maenner MJ, Baio J, et al. Early Identification of Autism Spectrum Disorder Among Children Aged 4 Years – Early Autism and Developmental Disabilities Monitoring Network, Six Sites, United States, 2016. MMWR Surveill Summ. 2020;69(3):1-11.
9. Wiggins LD, Durkin M, Esler A, et al. Disparities in Documented Diagnoses of Autism Spectrum Disorder Based on Demographic, Individual, and Service Factors. Autism Res. 2020;13(3):464-473.
10. Cheroni C, Caporale N, Testa G. Autism spectrum disorder at the crossroad between genes and environment: contributions, convergences, and interactions in ASD developmental pathophysiology. Mol Autism. 2020;11(1):69.
11. Hollander JA, Cory-Slechta DA, Jacka FN, et al. Beyond the looking glass: recent advances in understanding the impact of environmental exposures on neuropsychiatric disease. Neuropsychopharmacology. 2020;45(7):1086-1096.
12. Constantino JN, Abbacchi AM, Saulnier C, et al. Timing of the Diagnosis of Autism in African American Children. Pediatrics. 2020;146(3).
13. Smith KA, Gehricke JG, Iadarola S, Wolfe A, Kuhlthau KA. Disparities in Service Use Among Children With Autism: A Systematic Review. Pediatrics. 2020;145(Suppl 1):S35-S46.
14. Kim I, Dababnah S, Lee J. The Influence of Race and Ethnicity on the Relationship between Family Resilience and Parenting Stress in Caregivers of Children with Autism. J Autism Dev Disord. 2020;50(2):650-658.
15. Harris JF, Coffield CN, Janvier YM, Mandell D, Cidav Z. Validation of The Developmental Check-In Tool for Low-Literacy Autism Screening. Pediatrics. 2020.
16. Jones DR, Mandell DS. To address racial disparities in autism research, we must think globally, act locally. Autism. 2020;24(7):1587-1589.
17. Tran XA, McDonald N, Dickinson A, et al. Functional connectivity during language processing in 3-month-old infants at familial risk for autism spectrum disorder. Eur J Neurosci. 2020.
18. Dickinson A, Daniel M, Marin A, et al. Multivariate Neural Connectivity Patterns in Early Infancy Predict Later Autism Symptoms. Biol Psychiatry Cogn Neurosci Neuroimaging. 2020.
19. Jones EJH, Goodwin A, Orekhova E, et al. Infant EEG theta modulation predicts childhood intelligence. Sci Rep. 2020;10(1):11232.
20. Braithwaite EK, Jones EJH, Johnson MH, Holmboe K. Dynamic modulation of frontal theta power predicts cognitive ability in infancy. Dev Cogn Neurosci. 2020;45:100818.
21. Kellerman AM, Schwichtenberg AJ, Abu-Zhaya R, Miller M, Young GS, Ozonoff S. Dyadic Synchrony and Responsiveness in the First Year: Associations with Autism Risk. Autism Res. 2020.
22. Girault JB, Swanson MR, Meera SS, et al. Quantitative trait variation in ASD probands and toddler sibling outcomes at 24 months. J Neurodev Disord. 2020;12(1):5.
23. Wilkinson CL, Gabard-Durnam LJ, Kapur K, Tager-Flusberg H, Levin AR, Nelson CA. Use of longitudinal EEG measures in estimating language development in infants with and without familial risk for autism spectrum disorder. Neurobiol Lang (Camb). 2020;1(1):33-53.
24. Breuss MW, Antaki D, George RD, et al. Autism risk in offspring can be assessed through quantification of male sperm mosaicism. Nat Med. 2020;26(1):143-150.
25. Satterstrom FK, Kosmicki JA, Wang J, et al. Large-Scale Exome Sequencing Study Implicates Both Developmental and Functional Changes in the Neurobiology of Autism. Cell. 2020;180(3):568-584 e523.
26. Myers SM, Challman TD, Bernier R, et al. Insufficient Evidence for “Autism-Specific” Genes. Am J Hum Genet. 2020;106(5):587-595.
27. Harris HK, Sideridis GD, Barbaresi WJ, Harstad E. Pathogenic Yield of Genetic Testing in Autism Spectrum Disorder. Pediatrics. 2020;146(4).
28. Mordaunt CE, Jianu JM, Laufer BI, et al. Cord blood DNA methylome in newborns later diagnosed with autism spectrum disorder reflects early dysregulation of neurodevelopmental and X-linked genes. Genome Med. 2020;12(1):88.
29. Gui A, Jones EJH, Wong CCY, et al. Leveraging epigenetics to examine differences in developmental trajectories of social attention: A proof-of-principle study of DNA methylation in infants with older siblings with autism. Infant Behav Dev. 2020;60:101409.
30. Lyall K, Song L, Botteron K, et al. The Association Between Parental Age and Autism-Related Outcomes in Children at High Familial Risk for Autism. Autism Res. 2020;13(6):998-1010.
31. Chen S, Zhao S, Dalman C, Karlsson H, Gardner R. Association of maternal diabetes with neurodevelopmental disorders: autism spectrum disorders, attention-deficit/hyperactivity disorder and intellectual disability. Int J Epidemiol. 2020.
32. Corsi DJ, Donelle J, Sucha E, et al. Maternal cannabis use in pregnancy and child neurodevelopmental outcomes. Nat Med. 2020;26(10):1536-1540.
33. Berg EL, Pedersen LR, Pride MC, et al. Developmental exposure to near roadway pollution produces behavioral phenotypes relevant to neurodevelopmental disorders in juvenile rats. Transl Psychiatry. 2020;10(1):289.
34. Eggebrecht AT, Dworetsky A, Hawks Z, et al. Brain function distinguishes female carriers and non-carriers of familial risk for autism. Mol Autism. 2020;11(1):82.
35. Lunden JW, Durens M, Nestor J, et al. Development of a 3-D Organoid System Using Human Induced Pluripotent Stem Cells to Model Idiopathic Autism. Adv Neurobiol. 2020;25:259-297.
36. Adhya D, Swarup V, Nagy R, et al. Atypical Neurogenesis in Induced Pluripotent Stem Cells From Autistic Individuals. Biol Psychiatry. 2020.
37. DiCicco-Bloom EaM, J. Advances in Neurobiology. Switzerland: Springer; 2020.
38. Hanger B, Couch A, Rajendran L, Srivastava DP, Vernon AC. Emerging Developments in Human Induced Pluripotent Stem Cell-Derived Microglia: Implications for Modelling Psychiatric Disorders With a Neurodevelopmental Origin. Front Psychiatry. 2020;11:789.
39. Kaat AJ, Shui AM, Ghods SS, et al. Sex differences in scores on standardized measures of autism symptoms: a multisite integrative data analysis. J Child Psychol Psychiatry. 2020.
40. Ros-Demarize R, Bradley C, Kanne SM, et al. ASD symptoms in toddlers and preschoolers: An examination of sex differences. Autism Res. 2020;13(1):157-166.
41. Nayar K, Sealock JM, Maltman N, et al. Elevated Polygenic Burden for Autism Spectrum Disorder Is Associated With the Broad Autism Phenotype in Mothers of Individuals With Autism Spectrum Disorder. Biol Psychiatry. 2020.
42. Terloyeva D, Frey AJ, Park BY, et al. Meconium androgens are correlated with ASD-related phenotypic traits in early childhood in a familial enriched risk cohort. Mol Autism. 2020;11(1):93.
43. Fombonne E. Camouflage and autism. J Child Psychol Psychiatry. 2020;61(7):735-738.
44. Schwartz S, Wang L, Shinn-Cunningham BG, Tager-Flusberg H. Atypical Perception of Sounds in Minimally and Low Verbal Children and Adolescents With Autism as Revealed by Behavioral and Neural Measures. Autism Res. 2020;13(10):1718-1729.
45. Schwartz S, Wang L, Shinn-Cunningham BG, Tager-Flusberg H. Neural Evidence for Speech Processing Deficits During a Cocktail Party Scenario in Minimally and Low Verbal Adolescents and Young Adults with Autism. Autism Res. 2020.
46. Xie S, Karlsson H, Dalman C, et al. The Familial Risk of Autism Spectrum Disorder with and without Intellectual Disability. Autism Res. 2020.
47. McCauley JB, Pickles A, Huerta M, Lord C. Defining Positive Outcomes in More and Less Cognitively Able Autistic Adults. Autism Res. 2020.
48. Mingins JE, Tarver J, Waite J, Jones C, Surtees AD. Anxiety and intellectual functioning in autistic children: A systematic review and meta-analysis. Autism. 2020:1362361320953253.
49. McCauley JB, Elias R, Lord C. Trajectories of co-occurring psychopathology symptoms in autism from late childhood to adulthood. Dev Psychopathol. 2020;32(4):1287-1302.
50. James AC, Reardon T, Soler A, James G, Creswell C. Cognitive behavioural therapy for anxiety disorders in children and adolescents. Cochrane Database Syst Rev. 2020;11:CD013162.
51. Solish A, Klemencic N, Ritzema A, et al. Effectiveness of a modified group cognitive behavioral therapy program for anxiety in children with ASD delivered in a community context. Mol Autism. 2020;11(1):34.
52. Driscoll K, Schonberg M, Stark MF, Carter AS, Hirshfeld-Becker D. Family-Centered Cognitive Behavioral Therapy for Anxiety in Very Young Children with Autism Spectrum Disorder. J Autism Dev Disord. 2020;50(11):3905-3920.
53. Ehrenreich-May J, Simpson G, Stewart LM, et al. Treatment of anxiety in older adolescents and young adults with autism spectrum disorders: A pilot study. Bull Menninger Clin. 2020;84(2):105-136.
54. McBride NM, Weinzimmer SA, La Buissonniere-Ariza V, et al. The Impact of Comorbidity on Cognitive-Behavioral Therapy Response in Youth with Anxiety and Autism Spectrum Disorder. Child Psychiatry Hum Dev. 2020;51(4):625-635.
55. MacDuffie KE, Shen MD, Dager SR, et al. Sleep Onset Problems and Subcortical Development in Infants Later Diagnosed With Autism Spectrum Disorder. Am J Psychiatry. 2020;177(6):518-525.
56. Hornberg H, Perez-Garci E, Schreiner D, et al. Rescue of oxytocin response and social behaviour in a mouse model of autism. Nature. 2020;584(7820):252-256.
57. Mazurek MO, Parker RA, Chan J, Kuhlthau K, Sohl K, Collaborative EA. Effectiveness of the Extension for Community Health Outcomes Model as Applied to Primary Care for Autism: A Partial Stepped-Wedge Randomized Clinical Trial. JAMA Pediatr. 2020;174(5):e196306.
58. Bellesheim KR, Kizzee RL, Curran A, Sohl K. ECHO Autism: Integrating Maintenance of Certification with Extension for Community Healthcare Outcomes Improves Developmental Screening. J Dev Behav Pediatr. 2020;41(6):420-427.
59. Dow D, Day TN, Kutta TJ, Nottke C, Wetherby AM. Screening for autism spectrum disorder in a naturalistic home setting using the systematic observation of red flags (SORF) at 18-24 months. Autism Res. 2020;13(1):122-133.
60. Carpenter KLH, Hahemi J, Campbell K, et al. Digital Behavioral Phenotyping Detects Atypical Pattern of Facial Expression in Toddlers with Autism. Autism Res. 2020.
61. Kelleher BL, Halligan T, Witthuhn N, Neo WS, Hamrick L, Abbeduto L. Bringing the Laboratory Home: PANDABox Telehealth-Based Assessment of Neurodevelopmental Risk in Children. Front Psychol. 2020;11:1634.
By Alycia Halladay, PhD, Chief Science Officer and The Scientific Advisory Board of ASF
The ASF Yearly Summary of Science highlights major research accomplishments that directly affect the lives of families with autism spectrum disorder (ASD). These accomplishments impact families in a number of ways: by affording those diagnosed and their families a better understanding of a particular behavior or biological feature; identifying beneficial treatment targets, interventions, services or resources; discovering technologies that not only identify unique characteristics of people with ASD but also offer insight as to how to better serve that population and by offering future predictions.
ASD research continues to be challenged by clinical heterogeneity, a scientific term applied to the variability of symptoms found in subjects across the spectrum. Current research has identified increased diversity amongst people with autism participating in research; in turn, this has led to a reduction across time in differences between people with a diagnosis vs. those without a diagnosis1. In other words, those participating in research now show less severe features of ASD compared to 20 years ago. This reflects the inclusion of a more diverse set of people with autism, however, those on the more profoundly affected end may not see the benefits of research that predominantly includes those with completely different features of ASD. One solution proffered to rectify this challenge has been to stratify individuals with ASD into different groups for the purposes of research. Although advocates report that stratification lends itself to precisely determining the needs of specific groups and individuals, other researchers continue to cluster individuals into one group. Whether to stratify or cluster is a prominent discussion amongst scientists and advocates and could become polarizing, as both approaches affect research, basic nomenclature, services such as housing and employment and support services.
Features in infancy predict adult outcomes
Multiple studies this year have linked children’s symptoms and biology in infancy to later outcomes. Motor abilities, family history, brain connectivity all can independently contribute to how a child develops over time. These outcomes include an autism diagnosis, verbal ability, and cognition in adulthood. This sort of research can be used to help prepare families and customize interventions that focus on the most debilitating symptoms of ASD.
This year, to make predictions about future ASD features, more studies used a longitudinal study design. This design is critical to autism research because it follows a group comprised of individuals diagnosed with ASD and, at times, individuals without a diagnosis in order to determine how they are affected as adolescents and adults. Whereas a longitudinal study can be expensive, complex and does not produce immediate results, the nature of its design provides clinicians invaluable data, affording deeper insights that allow them to more fully educate families by managing expectations, identifying focus areas and providing coping strategies that serve to help those with ASD live their best lives.
Longitudinal studies help parents understand their child’s reality and manage future expectations, as well as help scientists refine interventions according to the variability of groups of people with ASD. Multiple research studies have used data to group children based on trajectory, i.e. the progression from commencement, through adolescent development to adult functioning. The composition of these groups consists of those who show fewer symptoms and continue to improve vs. those less functioning who continue to decline. This year, two longitudinal studies, one conducted in the United States and one in Canada, closely examined toddlers to pinpoint and study specific factors that influence outcomes, from childhood to adulthood. In these studies, two patterns emerged: those possessing lower levels of symptoms who improve vs. those with more profound symptoms who decline.
While all groups showed improvement in daily living skills, those who presented less severe symptoms in toddlerhood and showed marked progression during adolescence also had the highest adaptive abilities as adults2. Although most participants showed improvement in social communication with age, improvement varied, based on individual language ability as toddlers. Social communication impairments in 19 year olds was found to correlate with differences in language ability as early as age two. As speech improved, so did this core symptom of ASD3: those with early minimal language ability showed the greatest functioning impairments as adults. Likewise, fine motor skills in infancy4 is a predictor of language at age 19, in that better fine motor skills in early childhood is a predictor of better command of language in adulthood. Together, these findings demonstrate that poor early motor skills and decreased language function are related to later ASD symptoms. This is a crucial identification, considering that both fine motor skills and language are target areas of early intervention and that intervention may improve ASD through adulthood.
The study of early motor function is not only vital to further understanding how it affects those diagnosed, it also offers insight pre-diagnosis in terms of how early motor function may predict a later ASD diagnosis. The Baby Siblings Research Consortium (BSRC) is a group of researchers that studies initial features of ASD in siblings of children with ASD as young as 6 weeks of age. Siblings of children with ASD have a 15x greater probability of having ASD themselves than do other children. Similar to previously mentioned studies, BSRC also concludes that fine motor abilities at 6 months can predict an ASD diagnosis in siblings and expressive language ability in younger siblings at 3 years6,7.
Another factor BSRC researchers have employed to estimate the probability of diagnosis in children is number of siblings previously diagnosed with ASD. Those with at least 2 older siblings with ASD were found to have a higher probability of a diagnosis, as well as increased severe cognitive disabilities8. Based on family history, this information is vital in helping families better understand the probability of an ASD diagnosis in future children, as well as predicting strengths and limitations future children may face.
In addition to identifying behavioral markers, the past decade of research has revealed a blossoming of early biological factors that may serve as additional predictors of diagnosis, ranging from genetic tests9, salivary hormone markers and other reflections of altered development. Studies of brain structure, activity and connectivity have also proven valuable; when measured non-invasively, identified changes in activity in the frontal lobe of the brain during the first year of life have served to predict an ASD diagnosis in infant siblings10. Because brain wavelengths vary, identifying and monitoring changes in the size of each different type of wavelength over the course of a year serves as valuable information in terms of not just determining an ASD diagnosis but also for further understanding brain fluctuations during that time period10.
Complementary to brain activity, previous studies from the Infant Brain Imaging Network (IBIS) revealed different approaches to more accurately predicting ASD diagnosis by using measurements of brain structure and connectivity, in addition to mathematical algorithms based on the shape and function of different brain regions, as potential predictors of a later diagnosis. This year, the analysis of early brain based ASD markers has afforded scientists more precision in determining an association with brain connectivity in critical ASD brain regions, as well as an insistence on sameness and stereotyped behaviors at 12 – 24 months11. Not only do these biological based markers aide in predicting later diagnosis and identifying features of ASD within a diagnosis, they have the potential to serve as objective ways to help determine specific interventions, both medical and behavioral.
2. Screening is not perfect, but it is essential
New technologies contribute to greater use of standardized measures in different community settings. At the same time, clinicians and scientists have developed new ways to use common records and tools, resulting in better identification of concerns at even earlier stages. Families and care providers should confidently screen early and often.
Biological based markers hold promise for even earlier detection of features, especially in those with a family history. However, to make predictions about not just a diagnosis but future expectations of needs as well, most care providers, physicians and clinicians rely on behavioral concerns. Right now, most families lack access to EEG machines and MRIs and expensive genetic testing is most often not covered by insurance. The reality of early detection of ASD in 2019 is that it occurs mostly in primary care settings, where physicians help to interpret results for the family. In 2019, the AAP published an update to their 2007 guidelines for screening for autism and it continues to recommend autism-specific screening at 18 and 24 months12. Researchers continue to explore new ways to make this tool more accessible via technology, such as electronic tablets, whereas scientists continue to refine and improve accuracy screening tools using machine learning13.
One challenge of current screening practices (and in fact, in all of ASD research) is the disparity in screening and screening results amongst distinct racial and ethnic groups14. In order to address these differences, scientists are analyzing a variety of approaches fashioned to deal with these disparities and to increase access to screening tools. This includes remotely employing video based tools to capture ASD features to help identify and diagnosis ASD15-17. These video based tools help parents identify signs by providing real life examples of parent-child interactions18 and by examining existing reports of developmental milestones from electronic medical records19, with the goal of identifying early signs of developmental concerns as soon as possible, in as many infants as possible, regardless of race or ethnicity . Doing so will increase early diagnosis, leading to earlier intervention and increased understanding of ASD, self-awareness of symptoms and long-term improvement of services.
3. The lifespan of mental health challenges sparks new intervention possibilities
The high rate of mental health disorders in both children and adults with ASD means that a large percentage of this population and their families are burdened with enormous challenges Training community providers to deliver mental health interventions shows promise for alleviating these comorbidities. Clinicians need to be on the lookout for these psychiatric issues so people with autism receive the much-needed services they deserve.
While the core symptoms of ASD often lead to challenges in daily functioning, across the lifetime and spectrum of many individuals with ASD, co-occurring mental health conditions are a huge concern. Several older but smaller international studies provide a wide range of estimates of the prevalence of co-occurring conditions. A met- analysis and systematic review of these studies conducted in 2019 has helped to decipher the findings20. The findings revealed 28% comorbidity of ADHD (higher in kids than adults), 20% for anxiety disorders, 11% for depression and 9% for obsessive-compulsive disorder20. There is even overlap in brain based profiles of different diagnoses, both in terms of genetic activity21 and structure22. These mental health issues, particularly anxiety, can lead to an acute crisis requiring hospitalization23. Unfortunately, clinicians have limited knowledge and understanding of the nature of these mental health conditions in ASD24, making intervention difficult. However, ASD researchers have had luck training community mental health providers to deliver interventions focused on addressing these mental health challenges25. Training community based providers is a move in a promising direction, allowing more people to receive services in a variety of settings, but the efficacy of these interventions still lags behind those delivered in clinics26. Understanding the high co-occurrence of mental health issues helps families and individuals both plan for later health care needs and anticipate potential mental health problems before they occur.
4. Heritable factors that influence brain development result in multiple psychiatric conditions, including autism.
Researchers have determined that of the over 100 autism genes that exist, all act on early developmental functions and lead to diverse, overlapping outcomes, including psychiatric disorders, autism, and related conditions. Some genetic influences, while rare, can help define the mechanisms that lead to brain cells in autism developing over time. Although a link has been established connecting environmental influences to this same spectrum of conditions, few studies have successfully defined their interaction. These findings have implications for interventions and could lead to strategies for mitigating symptoms.
Given the comorbidity of mental health disorders with autism spectrum disorder, it should come as no surprise that new research reveals that ASD relevant genes act in fundamental ways that may influence multiple outcomes, ranging from ASD to schizophrenia, to ADHD27-30, neurodevelopmental disorders and intellectual disability31-33. Genes that act on such early and fundamental brain pathways have downstream effects on a number of brain functions, ASD being one of them. This might explain why there are so many ASD genes and why they are pleiotropic, meaning they have different functions. In fact, the list of genes associated with ASD keeps growing, as larger studies and better technology have revealed over 150 ASD associated genes34. Infant siblings of children with autism also show rare and common gene variants in ASD genes that can aid in a diagnosis9.
In addition, the presence of certain genetic mutations in ASD relevant genes can produce profound disabilities, which alone work to explain an ASD diagnosis. These mutations, referred to as rare genetic variants, are important to the community because their discovery has led to the creation of Patient Advocacy Groups that provide support and resources for focused research, as well as offer pathways to better understanding the basic circuitry of certain ASD behaviors35. Scientists are studying these rare genetic forms of ASD to understand all forms of ASD, particularly gene expression in the brain36,37. When compared to studies of the brains of people with bipolar disorder and schizophrenia, studies of brain tissue in people with ASD reveal overlapping genetic activity in genes that control synaptic signaling, neurotransmitter release, and immune response.36,37. The abnormal immune signaling in the brain might result in cell damage, as evidenced by accumulation of T-cells in brain tissue38. Studying the brains of people with ASD is the best way to understand the basic cellular and molecular basis of ASD, and is only possible through families who decide at the most difficult time to make the decision to donate. If you would like to learn more about the Autism BrainNet, which made these studies possible, visit www.takesbrains.org/signup.
While genetic factors are incredibly important in the diagnosis and presentation of symptoms of ASD, understanding the role of environmental factors in both the diagnosis and presentation of symptoms of ASD is crucial. One of the most studied environmental factors in ASD is exposure to air pollution during pregnancy. This year, ancillary evidence taken from additional locations via different methodologies shows a particular effect for a component in air pollution called PM (particulate matter) 2.5 (2.5 microns)39. Air pollution exposure may interact with maternal diabetes, which also increases the probability of ASD40. Air pollution also seems to influence an ASD diagnosis more strongly in boys41. It is important that public health policy address established, scientifically based environmental factors to address even smaller, but preventable, environmental factors.
There have been spurious reports of other environmental factors, but rather than look at factors in isolation, it is crucial to understand how these factors collectively influence brain development and interact with genetic susceptibility, either rare genetic or polygenic influences36. Another area of convergence of environmental and genetic factors is epigenetics, often called the “second genome”. The epigenome is a multitude of chemicals and tags on the DNA genome that is responsive to environmental factors that can turn on or turn off DNA expression, as early as when the embryo is formed. ASD risk genes identified in genetic studies can also work epigenetically42-46. The next generation of research will hopefully focus on understanding the multifactorial influences of an ASD diagnosis, how these factors affect symptoms and influence long term trajectories across neuropsychiatric diagnoses, including ASD.
5. Females with autism present features differently
Females with autism show opposite neurobiological features of autism, while also possessing some of the same core features of ASD. In females, these differences may be found in the way symptoms present or in associated features of ASD. Lack of differentiation clouds important scientific discoveries, which is why treatments and services should be sex specific.
Over the past five years, ASD research has increasingly focused more attention on identifying and understanding how autism manifests in females; this includes, but is not limited, to: genetic makeup, symptom presentation, long term trajectory and mental health issues. Females are diagnosed 4x less often but also have an increased load of genetic mutations, including recessive mutations47. This year, results of studies have been mixed in terms of the magnitude and nature of sex and gender related symptom presentation in males vs. females, noting a problem plaguing ASD research mentioned earlier: heterogeneity48. Differences across sex and gender are not seen in terms of presence or absence of symptoms, but rather in the way they present across different ages49,50. On the whole, differences are few in infants and toddlers but are magnified during adolescence, even in the way people perceive ASD symptoms in males and females51. Some scientists suggest that associated symptoms are most likely to present differently than core symptoms of ASD52, with females showing a higher prevalence of ADHD53 and OCD, leading to differences in the way males and females appear.
In addition to findings of increased numbers of recessive mutations in the genome of females47, analysis of brain structure has revealed sex differences further suggestive of the female protective effect. Focused study of the cerebellum has revealed that female activation patterns oppose those of males with ASD 54 and fail to evince similar patterns of connectivity across different brain regions55,56, i.e. females with ASD show reduced connectivity compared to females without ASD, an effect not seen in males with ASD55. In addition, when comparing twins, females had more profound differences in the sizes of brain regions compared to males57. These findings have led researchers to refine how they examine the role gender plays in basic science research.
Animal model research suggests that environmental exposures may not produce the same impairments in male vs. female offspring58. Taken together, these biological findings demonstrate that females, despite demonstrating a lower prevalence of ASD, also show complicated behavioral features and more biological markers for ASD. Future research must focus on why females are diagnosed less often than males and why, when they are diagnosed, they present more behavioral markers than their male counterparts.
6. It takes a village to make interventions work in the classroom
Teachers play a considerable role in identifying and helping kids across the spectrum, which is why teachers need focused training and support in order to best serve students with ASD.
Teachers and school administrators must perform a multitude of duties and responsibilities in an effort to meet the needs of students of varying abilities within the same classroom and provide all students – those on the spectrum and those who are not – with an equal opportunity to learn. In a perfect world, each student in our school systems would receive exactly what he or she needs, when it is needed, regardless of school systems and across different symptom presentation. Unfortunately, in 2019, researchers documented that in some states, the diagnosis of ASD does not necessarily correspond to the educational classification59, an inconsistency which might create disparities in service utilization across states, particularly considering that the quality of programs in many school systems rate just above adequate60.
Adding to these challenges in schools, research shows that students with ASD who exhibit unclear symptom presentation are likely to receive different services61,62. Teacher perception of what is effective often dictates what kind of evidence-based interventions are used in the school system63. Therefore, the specific types of support services students need in order to be successful often do not match up to what they actually receive. Studying clinic-based interventions in real world settings, such as in schools, is challenging as well. The biggest problem is that these interventions don’t always translate fluidly from clinic to classroom26 and often require modifications just to get them into the classroom. For example, according to research, a popular curriculum called TeachTown, commonly used by classroom teachers, does not necessarily help kids with ASD64. The good news is scientists are using opportunities like recess65 for social interventions in ASD.
Of real concern is that the types of educational based interventions can vary based on ethnic group66, leading to inequity in services. While racial and ethnic disparities continue to exist, researchers are exploring different methods to alleviate these differences. While Medicaid waivers have been shown to be somewhat helpful67, most research so far has focused more on defining the problem, so that future studies can be set up to address these challenges directly. Transition to employment in the school system can be improved by the perspectives of those that have successes and challenges with employment. This includes starting early and help build environmental supports for future success on the job68. These findings will lead to more tailored and effective intervention strategies to improve services for all people across the spectrum in schools, where they are desperately needed.
7. Model systems of autism are used to understand the earliest, fundamental features of ASD.
Scientists use animals and cells to determine what happens at the onset of autism and when it happens, beginning with the moment the cells are formed, in order to better build interventions for different times in development.
Animals do not have ASD. Cells in a dish do not have ASD. But animals and cells can still provide important insight into not just therapeutic targets but can also offer a comprehensive understanding on what is happening in the brains and bodies of people with ASD. The cells in a dish actually come from cells in a person, including those with idiopathic and rare genetic forms of ASD. By using induced pluripotent stem cell (iPSC) technologies to transform a skin cell into a brain cell and then back into a skin cell, important discoveries about individual brain development can emerge. These models have revealed that certain genes cause neurons to be overconnected69 while others can impair the strengths of those connections70 or reduce neuronal activity on the cellular level71. These are the basic fundamental properties of cell development that seem to be common across multiple psychiatric conditions, including autism.
In turn, animal models allow for a more complex analysis of single genes in the presence of organisms with other genes. Together with findings in brain tissue, these animal models have shown that, despite the gene involved, there are converging networks that could be the target of future interventions72. Animal models can also demonstrate which gene x environment interactions exacerbate symptoms or alleviate symptoms in a controlled setting73,74. They have also been able to identify the underlying molecular mechanisms of genetic mutations associated with ASD75,76. Beyond the brain, these new models can identify mechanisms of associated dysfunction like gastrointestinal functions75 which plague many families with ASD. A new technology introduced last year called CRISPR allows researchers to better target genes one at a time or in combination to better understand the roles of genes as well as gene x environment interactions on basic functioning of cells across the body and what this means for humans, helping them both understand and anticipate specific symptoms across time.
8. While scientists now know more about interventions, there is much that they still need to learn.
While the efficacy of fluoxetine for repetitive behaviors has been addressed, other treatments such as fecal transplants, stem cell transplants and cannabidiol still lack an evidence base and therefore use is not recommended at this time. The autism community should be cautious of interventions that lack strong scientific research, as well as by wary of flashy headlines
This year, advances in behavioral interventions for ASD revealed a common theme: remote delivery. This includes development of telehealth methods77 and videoconferencing78. As mentioned earlier, this methodology will expand coverage while striving to ensure quality. However, findings also demonstrated what does not work. For example, fluoxetine, or Prozac, has proved to be ineffective for repetitive behaviors in ASD79,80 however that does not mean people should go off of their medication if it is helping them in other areas, but instead they should be aware that it may not help the core symptoms of ASD. On the other hand, new research in other drug targets, including the vasopressin receptor, showed promise in males81. While more work needs to be done, scientists have a better understanding of what works for particular symptoms in specific people.
Although much is known, there is a great need to acknowledge emerging fields where little is known, especially in the field of intervention. Media reports hyping the effectiveness of stem cell studies and fecal transplants pushed these alternative treatments into public view however, the designs were subject to bias82 or had small sample sizes83, suggesting further caution when considering these alternative, non-evidence based approaches. On the other hand, the target of the fecal transplants, the microbiome, has been understudied in basic and clinical studies. Probiotics have also led to improvements in gastrointestinal function in people with ASD85, providing evidence that the microbiome is important but needs further study, both in determining mechanism in model systems and more precise intervention therapies.
Another alternative therapy used by families with no substantial scientific evidence is medical marijuana, including the psychoactive component THC and a non-psychoactive chemical within the cannabis plant called CBD. Unfortunately, again, media hype and marketing strategies have provided hope where scientific evidence is lacking. Research in this area is hampered by legal and administrative policies, but newer, more definitive research studies are in progress. While there is reason to be hopeful in this area, there is also reason to be cautious. People with ASD respond differently to CBD than those without ASD86, and parents should not assume what works in one child without ASD will work in their child with ASD.
The Autism Science Foundation recognizes that there is much scientific information available from multiple sources that can be accessed on multiple platforms. This summary is meant to highlight this year’s advances, including differences that have changed over time and across sex, as well as shed light on similarities with other neuropsychiatric disorders. It is hard for anyone to make sense of it all when it is announced, or even as these discoveries build on each other. However, it’s important to know that advancements in understanding the basic biology of ASD have led to more specific interventions, increased knowledge of what works and what does work, further expansion in utility across settings and lastly, clues for future studies. Although this summary does not capture every insight and advancement revealed in scientific studies of ASD this year, ASF feels that these highlights offer a comprehensive overview and it will continue to share science news throughout 2020, particularly what is most valuable in helping family members understand how to best serve loved ones with ASD and themselves.
References:
1. Rodgaard EM, Jensen K, Vergnes JN, Soulieres I, Mottron L. Temporal Changes in Effect Sizes of Studies Comparing Individuals With and Without Autism: A Meta-analysis. JAMA Psychiatry. 2019.
2. Di Rezze B, Duku E, Szatmari P, et al. Examining Trajectories of Daily Living Skills over the Preschool Years for Children with Autism Spectrum Disorder. J Autism Dev Disord. 2019;49(11):4390-4399.
3. Bal VH, Kim SH, Fok M, Lord C. Autism spectrum disorder symptoms from ages 2 to 19 years: Implications for diagnosing adolescents and young adults. Autism Res. 2019;12(1):89-99.
4. Bal VH, Fok M, Lord C, et al. Predictors of longer-term development of expressive language in two independent longitudinal cohorts of language-delayed preschoolers with Autism Spectrum Disorder. J Child Psychol Psychiatry. 2019.
5. Cain MK, Kaboski JR, Gilger JW. Profiles and academic trajectories of cognitively gifted children with autism spectrum disorder. Autism. 2019;23(7):1663-1674.
6. Iverson JM, Shic F, Wall CA, et al. Early motor abilities in infants at heightened versus low risk for ASD: A Baby Siblings Research Consortium (BSRC) study. J Abnorm Psychol. 2019;128(1):69-80.
7. LeBarton ES, Landa RJ. Infant motor skills predicts later expressive language and autism spectrum disorder diagnosis. Infant Behav Dev. 2019;54:37-47.
8. McDonald NM, Senturk D, Scheffler A, et al. Developmental Trajectories of Infants With Multiplex Family Risk for Autism: A Baby Siblings Research Consortium Study. JAMA Neurol. 2019.
9. D’Abate L, Walker S, Yuen RKC, et al. Predictive impact of rare genomic copy number variations in siblings of individuals with autism spectrum disorders. Nat Commun. 2019;10(1):5519.
10. Gabard-Durnam LJ, Wilkinson C, Kapur K, Tager-Flusberg H, Levin AR, Nelson CA. Longitudinal EEG power in the first postnatal year differentiates autism outcomes. Nat Commun. 2019;10(1):4188.
11. McKinnon CJ, Eggebrecht AT, Todorov A, et al. Restricted and Repetitive Behavior and Brain Functional Connectivity in Infants at Risk for Developing Autism Spectrum Disorder. Biol Psychiatry Cogn Neurosci Neuroimaging. 2019;4(1):50-61.
12. Hyman SL, Levy SE, Myers SM. Identification, Evaluation, and Management of Children With Autism Spectrum Disorder. Pediatrics. 2019:e20193447.
13. Achenie LEK, Scarpa A, Factor RS, Wang T, Robins DL, McCrickard DS. A Machine Learning Strategy for Autism Screening in Toddlers. J Dev Behav Pediatr. 2019;40(5):369-376.
14. Rea KE, Armstrong-Brine M, Ramirez L, Stancin T. Ethnic Disparities in Autism Spectrum Disorder Screening and Referral: Implications for Pediatric Practice. J Dev Behav Pediatr. 2019;40(7):493-500.
15. Egger HL, Dawson G, Hashemi J, et al. Automatic emotion and attention analysis of young children at home: a ResearchKit autism feasibility study. NPJ Digit Med. 2018;1:20.
16. Dawson G, Sapiro G. Potential for Digital Behavioral Measurement Tools to Transform the Detection and Diagnosis of Autism Spectrum Disorder. JAMA Pediatr. 2019;173(4):305-306.
17. Sabatos-DeVito M, Murias M, Dawson G, et al. Methodological considerations in the use of Noldus EthoVision XT video tracking of children with autism in multi-site studies. Biol Psychol. 2019;146:107712.
18. Young GS, Constantino JN, Dvorak S, et al. A video-based measure to identify autism risk in infancy. J Child Psychol Psychiatry. 2019.
19. Guthrie W, Wallis K, Bennett A, et al. Accuracy of Autism Screening in a Large Pediatric Network. Pediatrics. 2019;144(4).
20. Lai MC, Kassee C, Besney R, et al. Prevalence of co-occurring mental health diagnoses in the autism population: a systematic review and meta-analysis. Lancet Psychiatry. 2019;6(10):819-829.
21. Kushki A, Anagnostou E, Hammill C, et al. Examining overlap and homogeneity in ASD, ADHD, and OCD: a data-driven, diagnosis-agnostic approach. Transl Psychiatry. 2019;9(1):318.
22. Koshiyama D, Fukunaga M, Okada N, et al. White matter microstructural alterations across four major psychiatric disorders: mega-analysis study in 2937 individuals. Mol Psychiatry. 2019.
23. Vasa RA, Hagopian L, Kalb LG. Investigating Mental Health Crisis in Youth with Autism Spectrum Disorder. Autism Res. 2019.
24. Maddox BB, Crabbe S, Beidas RS, et al. “I wouldn’t know where to start”: Perspectives from clinicians, agency leaders, and autistic adults on improving community mental health services for autistic adults. Autism. 2019:1362361319882227.
25. Brookman-Frazee L, Roesch S, Chlebowski C, Baker-Ericzen M, Ganger W. Effectiveness of Training Therapists to Deliver An Individualized Mental Health Intervention for Children With ASD in Publicly Funded Mental Health Services: A Cluster Randomized Clinical Trial. JAMA Psychiatry. 2019;76(6):574-583.
26. Nahmias AS, Pellecchia M, Stahmer AC, Mandell DS. Effectiveness of community-based early intervention for children with autism spectrum disorder: a meta-analysis. J Child Psychol Psychiatry. 2019;60(11):1200-1209.
27. Forsyth JK, Nachun D, Gandal MJ, et al. Synaptic and Gene Regulatory Mechanisms in Schizophrenia, Autism, and 22q11.2 Copy Number Variant-Mediated Risk for Neuropsychiatric Disorders. Biol Psychiatry. 2019.
28. Schork AJ, Won H, Appadurai V, et al. A genome-wide association study of shared risk across psychiatric disorders implicates gene regulation during fetal neurodevelopment. Nat Neurosci. 2019;22(3):353-361.
29. Walker RL, Ramaswami G, Hartl C, et al. Genetic Control of Expression and Splicing in Developing Human Brain Informs Disease Mechanisms. Cell. 2019;179(3):750-771 e722.
30. Grove J, Ripke S, Als TD, et al. Identification of common genetic risk variants for autism spectrum disorder. Nat Genet. 2019;51(3):431-444.
31. Douzgou S, Liang HW, Metcalfe K, et al. The clinical presentation caused by truncating CHD8 variants. Clin Genet. 2019;96(1):72-84.
32. Clifford H, Dulneva A, Ponting CP, Haerty W, Becker EBE. A gene expression signature in developing Purkinje cells predicts autism and intellectual disability comorbidity status. Sci Rep. 2019;9(1):485.
33. Arnett AB, Rhoads CL, Hoekzema K, et al. The autism spectrum phenotype in ADNP syndrome. Autism Res. 2018;11(9):1300-1310.
34. Feliciano P, Zhou X, Astrovskaya I, et al. Exome sequencing of 457 autism families recruited online provides evidence for autism risk genes. NPJ Genom Med. 2019;4:19.
35. Sanders SJ, Sahin M, Hostyk J, et al. A framework for the investigation of rare genetic disorders in neuropsychiatry. Nat Med. 2019;25(10):1477-1487.
36. Wong CCY, Smith RG, Hannon E, et al. Genome-wide DNA methylation profiling identifies convergent molecular signatures associated with idiopathic and syndromic autism in post-mortem human brain tissue. Hum Mol Genet. 2019;28(13):2201-2211.
37. Guan J, Cai JJ, Ji G, Sham PC. Commonality in dysregulated expression of gene sets in cortical brains of individuals with autism, schizophrenia, and bipolar disorder. Transl Psychiatry. 2019;9(1):152.
38. DiStasio MM, Nagakura I, Nadler MJ, Anderson MP. T lymphocytes and cytotoxic astrocyte blebs correlate across autism brains. Ann Neurol. 2019;86(6):885-898.
39. McGuinn LA, Windham GC, Kalkbrenner AE, et al. Early Life Exposure to Air Pollution and Autism Spectrum Disorder: Findings from a Multisite Case-Control Study. Epidemiology. 2019.
40. Jo H, Eckel SP, Chen JC, et al. Gestational diabetes mellitus, prenatal air pollution exposure, and autism spectrum disorder. Environ Int. 2019;133(Pt A):105110.
41. Jo H, Eckel SP, Wang X, et al. Sex-specific associations of autism spectrum disorder with residential air pollution exposure in a large Southern California pregnancy cohort. Environ Pollut. 2019;254(Pt A):113010.
42. Sessa A, Fagnocchi L, Mastrototaro G, et al. SETD5 Regulates Chromatin Methylation State and Preserves Global Transcriptional Fidelity during Brain Development and Neuronal Wiring. Neuron. 2019;104(2):271-289 e213.
43. Siu MT, Butcher DT, Turinsky AL, et al. Functional DNA methylation signatures for autism spectrum disorder genomic risk loci: 16p11.2 deletions and CHD8 variants. Clin Epigenetics. 2019;11(1):103.
44. Vogel Ciernia A, Laufer BI, Hwang H, et al. Epigenomic Convergence of Neural-Immune Risk Factors in Neurodevelopmental Disorder Cortex. Cereb Cortex. 2019.
45. Saffari A, Arno M, Nasser E, et al. RNA sequencing of identical twins discordant for autism reveals blood-based signatures implicating immune and transcriptional dysregulation. Mol Autism. 2019;10:38.
46. Tremblay MW, Jiang YH. DNA Methylation and Susceptibility to Autism Spectrum Disorder. Annu Rev Med. 2019;70:151-166.
47. Doan RN, Lim ET, De Rubeis S, et al. Recessive gene disruptions in autism spectrum disorder. Nat Genet. 2019;51(7):1092-1098.
48. Mahendiran T, Brian J, Dupuis A, et al. Meta-Analysis of Sex Differences in Social and Communication Function in Children With Autism Spectrum Disorder and Attention-Deficit/Hyperactivity Disorder. Front Psychiatry. 2019;10:804.
49. Bitsika V, Sharpley CF. Effects of Diagnostic Severity upon Sex Differences in Behavioural Profiles of Young Males and Females with Autism Spectrum Disorder. J Autism Dev Disord. 2019;49(11):4429-4440.
50. Margari L, Palumbi R, Peschechera A, et al. Sex-Gender Comparisons in Comorbidities of Children and Adolescents With High-Functioning Autism Spectrum Disorder. Front Psychiatry. 2019;10:159.
51. Geelhand P, Bernard P, Klein O, van Tiel B, Kissine M. The role of gender in the perception of autism symptom severity and future behavioral development. Mol Autism. 2019;10:16.
52. Lundstrom S, Marland C, Kuja-Halkola R, et al. Assessing autism in females: The importance of a sex-specific comparison. Psychiatry Res. 2019:112566.
53. Ottosen C, Larsen JT, Faraone SV, et al. Sex Differences in Comorbidity Patterns of Attention-Deficit/Hyperactivity Disorder. J Am Acad Child Adolesc Psychiatry. 2019;58(4):412-422 e413.
54. Smith REW, Avery JA, Wallace GL, Kenworthy L, Gotts SJ, Martin A. Sex Differences in Resting-State Functional Connectivity of the Cerebellum in Autism Spectrum Disorder. Front Hum Neurosci. 2019;13:104.
55. Lei J, Lecarie E, Jurayj J, et al. Altered Neural Connectivity in Females, But Not Males with Autism: Preliminary Evidence for the Female Protective Effect from a Quality-Controlled Diffusion Tensor Imaging Study. Autism Res. 2019;12(10):1472-1483.
56. Andrews DS, Lee JK, Solomon M, Rogers SJ, Amaral DG, Nordahl CW. A diffusion-weighted imaging tract-based spatial statistics study of autism spectrum disorder in preschool-aged children. J Neurodev Disord. 2019;11(1):32.
57. Cauvet E, Van’t Westeinde A, Toro R, et al. Sex Differences Along the Autism Continuum: A Twin Study of Brain Structure. Cereb Cortex. 2019;29(3):1342-1350.
58. Carlezon WA, Jr., Kim W, Missig G, et al. Maternal and early postnatal immune activation produce sex-specific effects on autism-like behaviors and neuroimmune function in mice. Sci Rep. 2019;9(1):16928.
59. Maddox BB, Rump KM, Stahmer AC, et al. Concordance between a U.S. Educational Autism Classification and the Autism Diagnostic Observation Schedule. J Clin Child Adolesc Psychol. 2019:1-7.
60. Kraemer BR, Odom SL, Tomaszewski B, et al. Quality of high school programs for students with autism spectrum disorder. Autism. 2019:1362361319887280.
61. Rosen TE, Spaulding CJ, Gates JA, Lerner MD. Autism severity, co-occurring psychopathology, and intellectual functioning predict supportive school services for youth with autism spectrum disorder. Autism. 2019;23(7):1805-1816.
62. Nuske HJ, Pellecchia M, Lushin V, et al. Do Student Characteristics Affect Teachers’ Decisions to Use 1:1 Instruction? J Autism Dev Disord. 2019;49(7):2864-2872.
63. Locke J, Lawson GM, Beidas RS, et al. Individual and organizational factors that affect implementation of evidence-based practices for children with autism in public schools: a cross-sectional observational study. Implement Sci. 2019;14(1):29.
64. Pellecchia M, Marcus SC, Spaulding C, et al. Randomized Trial of a Computer-Assisted Intervention for Children With Autism in Schools. J Am Acad Child Adolesc Psychiatry. 2019.
65. Locke J, Kang-Yi C, Pellecchia M, Mandell DS. It’s Messy but Real: A Pilot Study of the Implementation a Social Engagement Intervention for Children with Autism in Schools. J Res Spec Educ Needs. 2019;19(2):135-144.
66. Bilaver LA, Havlicek J. Racial and Ethnic Disparities in Autism-Related Health and Educational Services. J Dev Behav Pediatr. 2019;40(7):501-510.
67. LaClair M, Mandell DS, Dick AW, Iskandarani K, Stein BD, Leslie DL. The effect of Medicaid waivers on ameliorating racial/ethnic disparities among children with autism. Health Serv Res. 2019;54(4):912-919.
68. Black MH, Mahdi S, Milbourn B, et al. Perspectives of key stakeholders on employment of autistic adults across the united states, australia, and sweden. Autism Res. 2019;12(11):1648-1662.
69. Zaslavsky K, Zhang WB, McCready FP, et al. SHANK2 mutations associated with autism spectrum disorder cause hyperconnectivity of human neurons. Nat Neurosci. 2019;22(4):556-564.
70. Ross PJ, Zhang WB, Mok RSF, et al. Synaptic Dysfunction in Human Neurons With Autism-Associated Deletions in PTCHD1-AS. Biol Psychiatry. 2019.
71. Deneault E, White SH, Rodrigues DC, et al. Complete Disruption of Autism-Susceptibility Genes by Gene Editing Predominantly Reduces Functional Connectivity of Isogenic Human Neurons. Stem Cell Reports. 2018;11(5):1211-1225.
72. Gordon A, Forsingdal A, Klewe IV, et al. Transcriptomic networks implicate neuronal energetic abnormalities in three mouse models harboring autism and schizophrenia-associated mutations. Mol Psychiatry. 2019.
73. Kim JW, Park K, Kang RJ, et al. Gene-environment interaction counterbalances social impairment in mouse models of autism. Sci Rep. 2019;9(1):11490.
74. Mohammadi S, Asadi-Shekaari M, Basiri M, Parvan M, Shabani M, Nozari M. Improvement of autistic-like behaviors in adult rats prenatally exposed to valproic acid through early suppression of NMDA receptor function. Psychopharmacology (Berl). 2019.
75. Tang S, Terzic B, Wang IJ, et al. Altered NMDAR signaling underlies autistic-like features in mouse models of CDKL5 deficiency disorder. Nat Commun. 2019;10(1):2655.
76. Xing X, Zhang J, Wu K, et al. Suppression of Akt-mTOR pathway rescued the social behavior in Cntnap2-deficient mice. Sci Rep. 2019;9(1):3041.
77. Talbott MR, Dufek S, Zwaigenbaum L, et al. Brief Report: Preliminary Feasibility of the TEDI: A Novel Parent-Administered Telehealth Assessment for Autism Spectrum Disorder Symptoms in the First Year of Life. J Autism Dev Disord. 2019.
78. Mazurek MO, Stobbe G, Loftin R, et al. ECHO Autism Transition: Enhancing healthcare for adolescents and young adults with autism spectrum disorder. Autism. 2019:1362361319879616.
79. Reddihough DS, Marraffa C, Mouti A, et al. Effect of Fluoxetine on Obsessive-Compulsive Behaviors in Children and Adolescents With Autism Spectrum Disorders: A Randomized Clinical Trial. JAMA. 2019;322(16):1561-1569.
80. Herscu P, Handen BL, Arnold LE, et al. The SOFIA Study: Negative Multi-center Study of Low Dose Fluoxetine on Repetitive Behaviors in Children and Adolescents with Autistic Disorder. J Autism Dev Disord. 2019.
81. Bolognani F, Del Valle Rubido M, Squassante L, et al. A phase 2 clinical trial of a vasopressin V1a receptor antagonist shows improved adaptive behaviors in men with autism spectrum disorder. Sci Transl Med. 2019;11(491).
82. Carpenter KLH, Major S, Tallman C, et al. White Matter Tract Changes Associated with Clinical Improvement in an Open-Label Trial Assessing Autologous Umbilical Cord Blood for Treatment of Young Children with Autism. Stem Cells Transl Med. 2019;8(2):138-147.
83. Kang DW, Adams JB, Coleman DM, et al. Long-term benefit of Microbiota Transfer Therapy on autism symptoms and gut microbiota. Sci Rep. 2019;9(1):5821.
84. Sharon G, Cruz NJ, Kang DW, et al. Human Gut Microbiota from Autism Spectrum Disorder Promote Behavioral Symptoms in Mice. Cell. 2019;177(6):1600-1618 e1617.
85. Arnold LE, Luna RA, Williams K, et al. Probiotics for Gastrointestinal Symptoms and Quality of Life in Autism: A Placebo-Controlled Pilot Trial. J Child Adolesc Psychopharmacol. 2019;29(9):659-669.
86. Pretzsch CM, Voinescu B, Mendez MA, et al. The effect of cannabidiol (CBD) on low-frequency activity and functional connectivity in the brain of adults with and without autism spectrum disorder (ASD). J Psychopharmacol. 2019;33(9):1141-1148.
On Tuesday, the journal Lancet published a 2+ year long endeavor around understanding the heterogeneity of autism not just in features but in access to services for individuals and families across the world. They called for a stepped care to help individualize and prioritize needs in different individuals based on their needs, not their diagnosis. They also called for the label of “profound autism” which describes individuals with very different outcomes compared to those who have a higher verbal and cognitive ability. Recognizing everyone needs supports and help, the “profound autism” label needs different supports, like different employment situations and different living accommodations. Thankfully, to authors, Dr. Catherine Lord from UCLA and Alison Singer from ASF explain the article and the impact they hope it makes on the field. Listen to the podcast here.